

Assessment of Systemic Delivery of rAAVrh74.MHCK7.micro-dystrophin in Children With Duchenne Muscular Dystrophy: A Nonrandomized Controlled Trial
- PMID: 32539076
- PMCID: PMC7296461
- DOI: 10.1001/jamaneurol.2020.1484
Assessment of Systemic Delivery of rAAVrh74.MHCK7.micro-dystrophin in Children With Duchenne Muscular Dystrophy: A Nonrandomized Controlled Trial
Abstract
Importance: Micro-dystrophin gene transfer shows promise for treating patients with Duchenne muscular dystrophy (DMD) using recombinant adeno-associated virus serotype rh74 (rAAVrh74) and codon-optimized human micro-dystrophin driven by a skeletal and cardiac muscle-specific promoter with enhanced cardiac expression (MHCK7).
Objective: To identify the 1-year safety and tolerability of intravenous rAAVrh74.MHCK7.micro-dystrophin in patients with DMD.
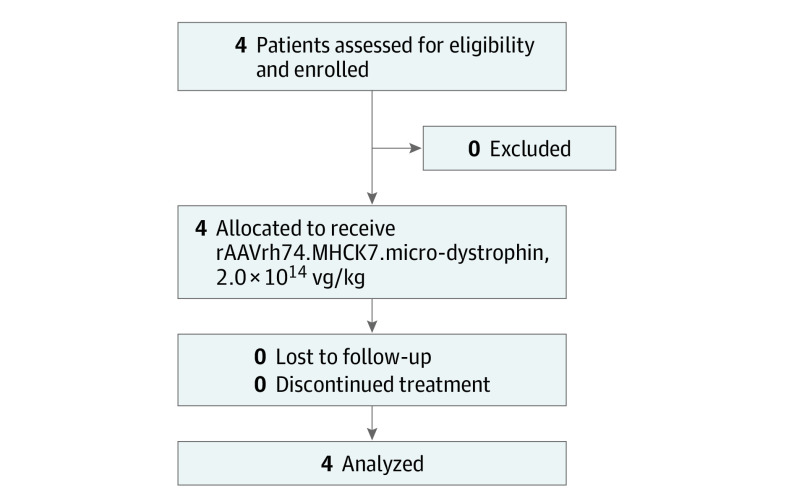
Design, setting, and participants: This open-label, phase 1/2a nonrandomized controlled trial was conducted at the Nationwide Children's Hospital in Columbus, Ohio. It began on November 2, 2017, with a planned duration of follow-up of 3 years, ending in March 2021. The first 4 patients who met eligibility criteria were enrolled, consisting of ambulatory male children with DMD without preexisting AAVrh74 antibodies and a stable corticosteroid dose (≥12 weeks).
Interventions: A single dose of 2.0 × 1014 vg/kg rAAVrh74.MHCK7.micro-dystrophin was infused through a peripheral limb vein. Daily prednisolone, 1 mg/kg, started 1 day before gene delivery (30-day taper after infusion).
Main outcomes and measures: Safety was the primary outcome. Secondary outcomes included micro-dystrophin expression by Western blot and immunohistochemistry. Functional outcomes measured by North Star Ambulatory Assessment (NSAA) and serum creatine kinase were exploratory outcomes.
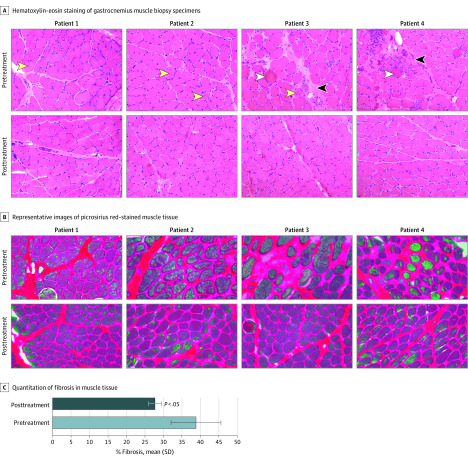
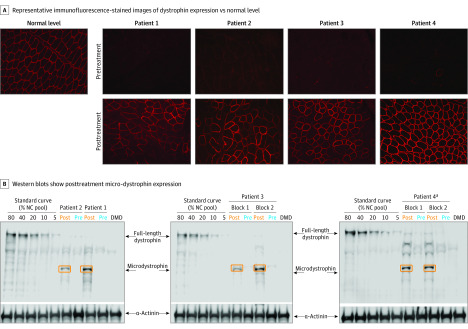
Results: Four patients were included (mean [SD] age at enrollment, 4.8 [1.0] years). All adverse events (n = 53) were considered mild (33 [62%]) or moderate (20 [38%]), and no serious adverse events occurred. Eighteen adverse events were considered treatment related, the most common of which was vomiting (9 of 18 events [50%]). Three patients had transiently elevated γ-glutamyltransferase, which resolved with corticosteroids. At 12 weeks, immunohistochemistry of gastrocnemius muscle biopsy specimens revealed robust transgene expression in all patients, with a mean of 81.2% of muscle fibers expressing micro-dystrophin with a mean intensity of 96% at the sarcolemma. Western blot showed a mean expression of 74.3% without fat or fibrosis adjustment and 95.8% with adjustment. All patients had confirmed vector transduction and showed functional improvement of NSAA scores and reduced creatine kinase levels (posttreatment vs baseline) that were maintained for 1 year.
Conclusions and relevance: This trial showed rAAVrh74.MHCK7.micro-dystrophin to be well tolerated and have minimal adverse events; the safe delivery of micro-dystrophin transgene; the robust expression and correct localization of micro-dystrophin protein; and improvements in creatine kinase levels and NSAA scores. These findings suggest that rAAVrh74.MHCK7.micro-dystrophin can provide functional improvement that is greater than that observed under standard of care.
Trial registration: ClinicalTrials.gov Identifier: NCT03375164.
Conflict of interest statement
Figures
References
-
- Birnkrant DJ, Bushby K, Bann CM, et al. ; DMD Care Considerations Working Group . Diagnosis and management of Duchenne muscular dystrophy, part 3: primary care, emergency management, psychosocial care, and transitions of care across the lifespan. Lancet Neurol. 2018;17(5):445-455. doi:10.1016/S1474-4422(18)30026-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
