

Hookworm Treatment for Relapsing Multiple Sclerosis: A Randomized Double-Blinded Placebo-Controlled Trial
- PMID: 32539079
- PMCID: PMC7296452
- DOI: 10.1001/jamaneurol.2020.1118
Hookworm Treatment for Relapsing Multiple Sclerosis: A Randomized Double-Blinded Placebo-Controlled Trial
Abstract
Importance: Studies suggest gut worms induce immune responses that can protect against multiple sclerosis (MS). To our knowledge, there are no controlled treatment trials with helminth in MS.
Objective: To determine whether hookworm treatment has effects on magnetic resonance imaging (MRI) activity and T regulatory cells in relapsing MS.
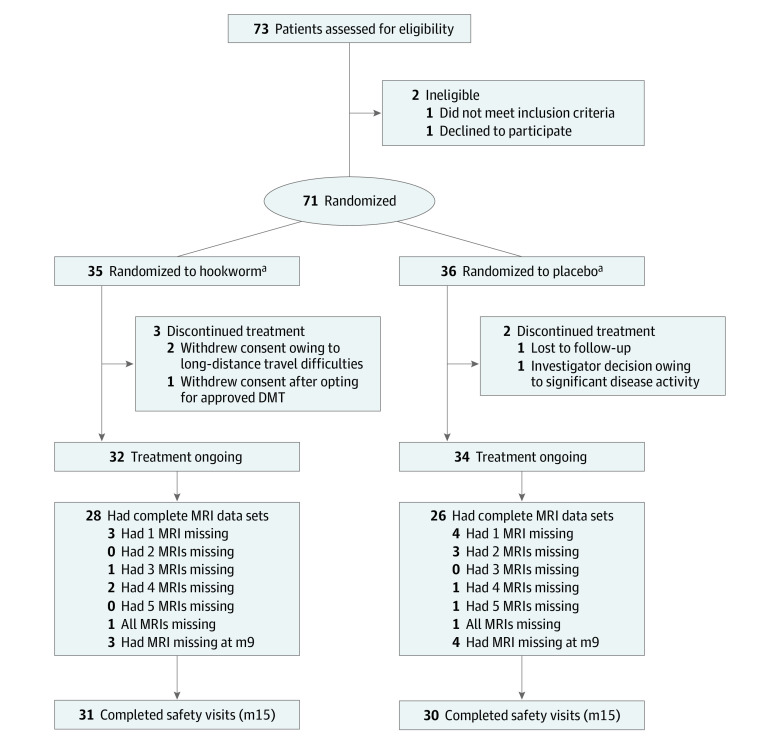
Design, setting, and participants: This 9-month double-blind, randomized, placebo-controlled trial was conducted between September 2012 and March 2016 in a modified intention-to-treat population (the data were analyzed June 2018) at the University of Nottingham, Queen's Medical Centre, a single tertiary referral center. Patients aged 18 to 61 years with relapsing MS without disease-modifying treatment were recruited from the MS clinic. Seventy-three patients were screened; of these, 71 were recruited (2 ineligible/declined).
Interventions: Patients were randomized (1:1) to receive either 25 Necator americanus larvae transcutaneously or placebo. The MRI scans were performed monthly during months 3 to 9 and 3 months posttreatment.
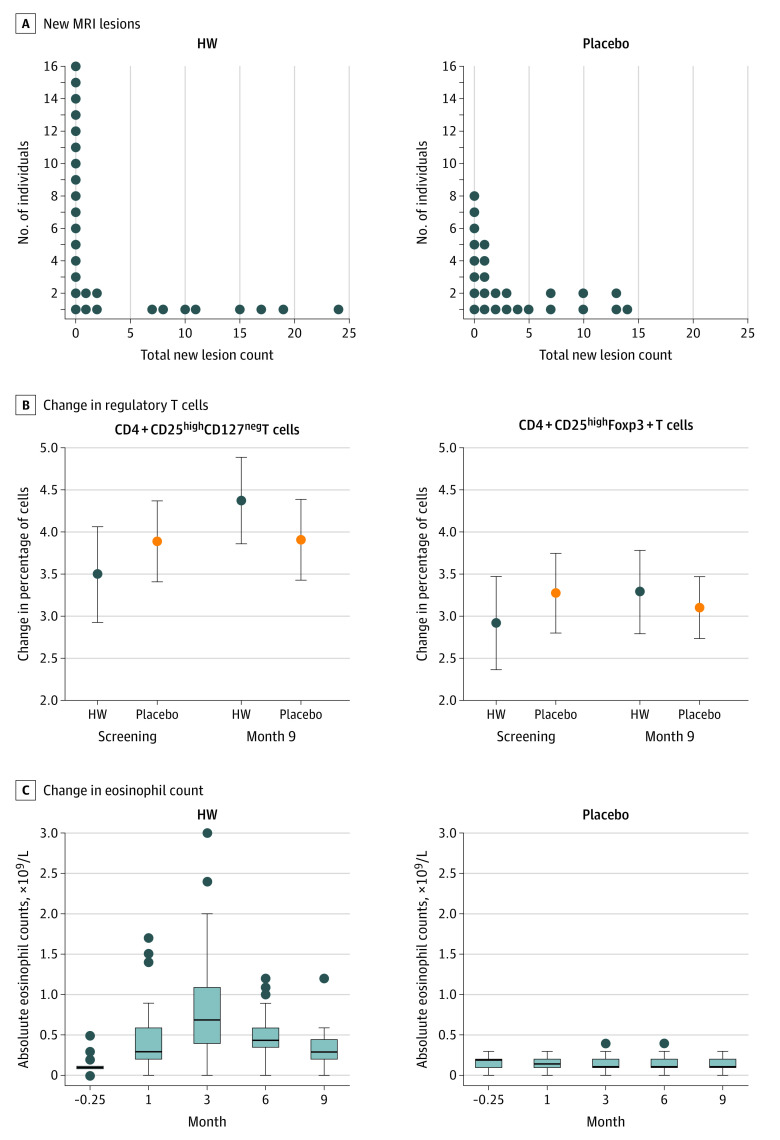
Main outcomes and measures: The primary end point was the cumulative number of new/enlarging T2/new enhancing T1 lesions at month 9. The secondary end point was the percentage of cluster of differentiation (CD) 4+CD25highCD127negT regulatory cells in peripheral blood.
Results: Patients (mean [SD] age, 45 [9.5] years; 50 women [71%]) were randomized to receive hookworm (35 [49.3%]) or placebo (36 [50.7%]). Sixty-six patients (93.0%) completed the trial. The median cumulative numbers of new/enlarging/enhancing lesions were not significantly different between the groups by preplanned Mann-Whitney U tests, which lose power with tied data (high number of zeroactivity MRIs in the hookworm group, 18/35 [51.4%] vs 10/36 [27.8%] in the placebo group). The percentage of CD4+CD25highCD127negT cells increased at month 9 in the hookworm group (hookworm, 32 [4.4%]; placebo, 34 [3.9%]; P = .01). No patients withdrew because of adverse effects. There were no differences in adverse events between groups except more application-site skin discomfort in the hookworm group (82% vs 28%). There were 5 relapses (14.3%) in the hookworm group vs 11 (30.6%) receiving placebo.
Conclusions and relevance: Treatment with hookworm was safe and well tolerated. The primary outcome did not reach significance, likely because of a low level of disease activity. Hookworm infection increased T regulatory cells, suggesting an immunobiological effect of hookworm. It appears that a living organism can precipitate immunoregulatory changes that may affect MS disease activity.
Trial registration: ClinicalTrials.gov Identifier: NCT01470521.
Conflict of interest statement
Figures
Comment in
-
Keep the Worms in the Mud.JAMA Neurol. 2020 Sep 1;77(9):1066-1067. doi: 10.1001/jamaneurol.2020.0519. JAMA Neurol. 2020. PMID: 32539129 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
