

Association Between Healthy Eating Patterns and Risk of Cardiovascular Disease
- PMID: 32539102
- PMCID: PMC7296454
- DOI: 10.1001/jamainternmed.2020.2176
Association Between Healthy Eating Patterns and Risk of Cardiovascular Disease
Abstract
Importance: The 2015-2020 Dietary Guidelines for Americans recommend multiple healthy eating patterns. However, few studies have examined the associations of adherence to different dietary patterns with long-term risk of cardiovascular disease (CVD).
Objective: To examine the associations of dietary scores for 4 healthy eating patterns with risk of incident CVD.
Design, setting, and participants: Prospective cohort study of initially healthy women from the Nurses' Health Study (NHS) (1984-2016) and the NHS II (1991-2017) and men from the Health Professionals Follow-up Study (HPFS) (1986-2012). The dates of analysis were July 25 to December 4, 2019.
Exposures: Healthy Eating Index-2015 (HEI-2015), Alternate Mediterranean Diet Score (AMED), Healthful Plant-Based Diet Index (HPDI), and Alternate Healthy Eating Index (AHEI).
Main outcomes and measures: Cardiovascular disease events, including fatal and nonfatal coronary heart disease (CHD) and stroke.
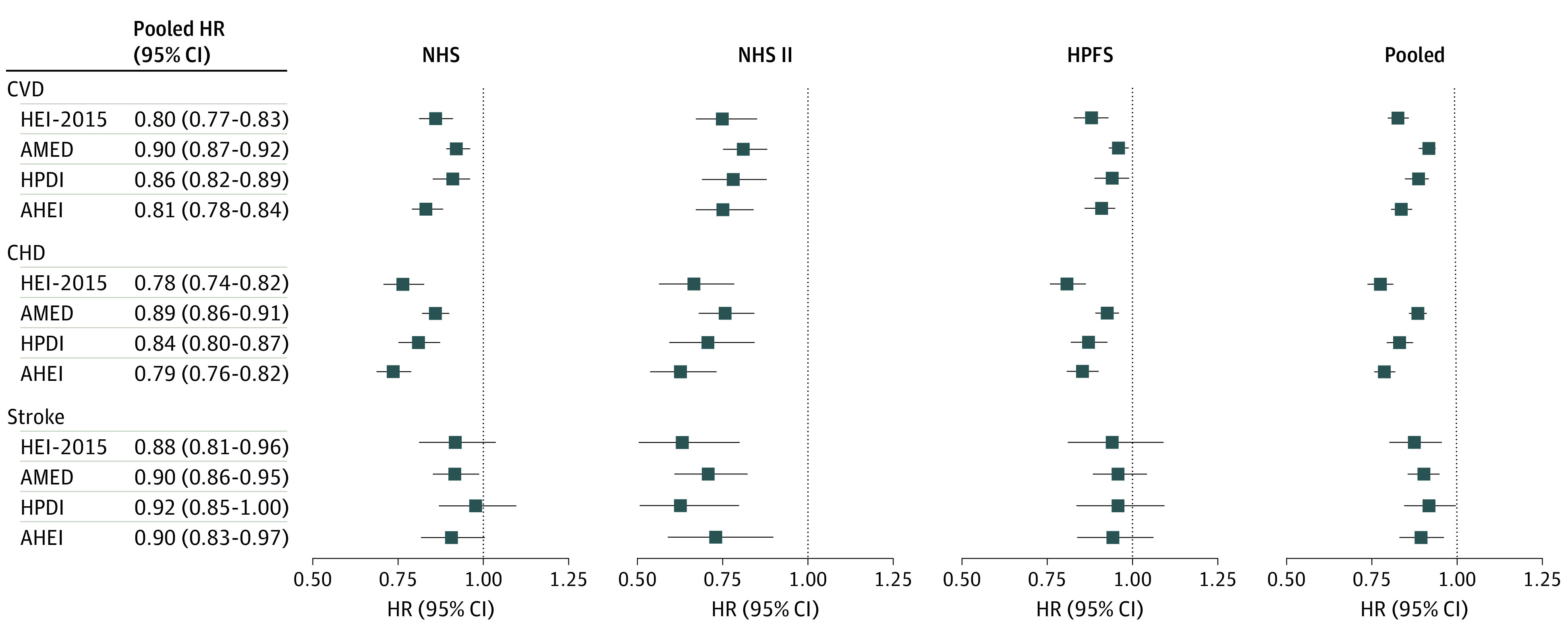
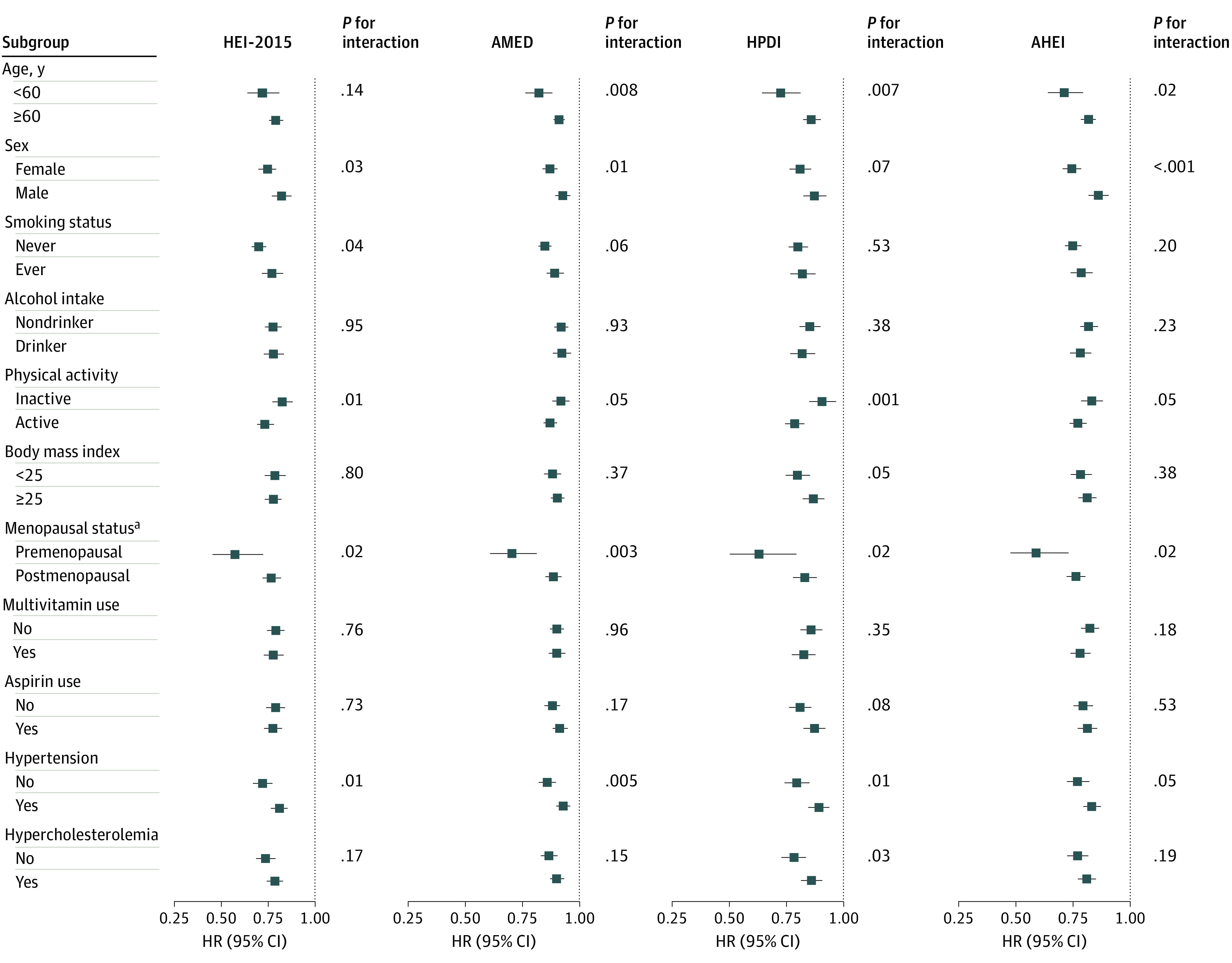
Results: The final study sample included 74 930 women in the NHS (mean [SD] baseline age, 50.2 [7.2] years), 90 864 women in the NHS II (mean [SD] baseline age, 36.1 [4.7] years), and 43 339 men in the HPFS (mean [SD] baseline age, 53.2 [9.6] years). During a total of 5 257 190 person-years of follow-up, 23 366 incident CVD cases were documented (18 092 CHD and 5687 stroke) (some individuals were diagnosed as having both CHD and stroke). Comparing the highest with the lowest quintiles, the pooled multivariable-adjusted hazard ratios (HRs) of CVD were 0.83 (95% CI, 0.79-0.86) for the HEI-2015, 0.83 (95% CI, 0.79-0.86) for the AMED, 0.86 (95% CI, 0.82-0.89) for the HPDI, and 0.79 (95% CI, 0.75-0.82) for the AHEI (P for trend <.001 for all). In addition, a 25-percentile higher dietary score was associated with 10% to 20% lower risk of CVD (pooled HR, 0.80 [95% CI, 0.77-0.83] for the HEI-2015; 0.90 [95% CI, 0.87-0.92] for the AMED; 0.86 [95% CI, 0.82-0.89] for the HPDI; and 0.81 [95% CI, 0.78-0.84] for the AHEI). These dietary scores were statistically significantly associated with lower risk of both CHD and stroke. In analyses stratified by race/ethnicity and other potential risk factors for CVD, the inverse associations between these scores and risk of CVD were consistent in most subgroups.
Conclusions and relevance: In 3 large prospective cohorts with up to 32 years of follow-up, greater adherence to various healthy eating patterns was consistently associated with lower risk of CVD. These findings support the recommendations of the 2015-2020 Dietary Guidelines for Americans that multiple healthy eating patterns can be adapted to individual food traditions and preferences.
Conflict of interest statement
Figures
Comment in
-
Ernährungsmuster relevanter als einzelne Nährstoffe : Kardiovaskuläre Gesundheit.MMW Fortschr Med. 2020 Aug;162(14):24-25. doi: 10.1007/s15006-020-0733-z. MMW Fortschr Med. 2020. PMID: 32780393 Review. German. No abstract available.
-
Nurses' awareness of diverse healthy diets may increase patients' adherence improving cardiovascular disease risk management.Evid Based Nurs. 2022 Jan;25(1):19. doi: 10.1136/ebnurs-2020-103329. Epub 2020 Dec 1. Evid Based Nurs. 2022. PMID: 33262167 No abstract available.
References
-
- Benjamin EJ, Muntner P, Alonso A, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics–2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56-e528. doi:10.1161/CIR.0000000000000659 - DOI - PubMed
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 [published correction appears in Lancet. 2019;393(10190):e44]. Lancet. 2018;392(10159):1789-1858. doi:10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
