

Genetic risk prediction of the plasma triglyceride response to independent supplementations with eicosapentaenoic and docosahexaenoic acids: the ComparED Study
- PMID: 32539794
- PMCID: PMC7294612
- DOI: 10.1186/s12263-020-00669-x
Genetic risk prediction of the plasma triglyceride response to independent supplementations with eicosapentaenoic and docosahexaenoic acids: the ComparED Study
Abstract
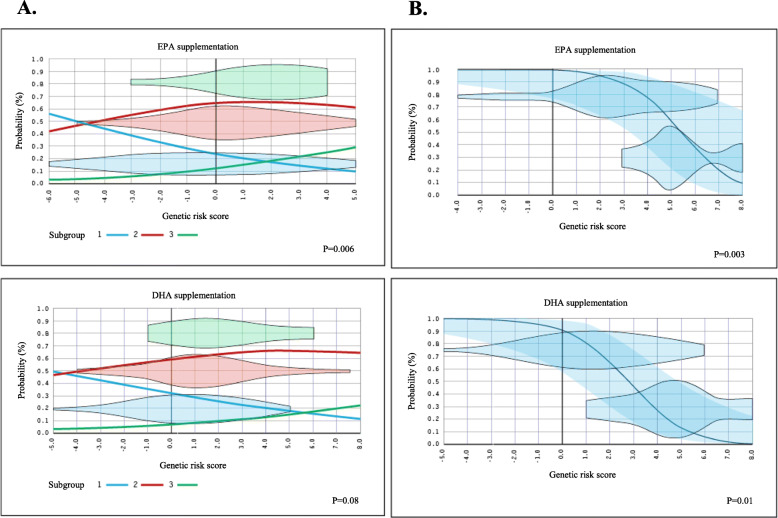
Background: We previously built a genetic risk score (GRS) highly predictive of the plasma triglyceride (TG) response to an omega-3 fatty acid (n-3 FA) supplementation from marine sources. The objective of the present study was to test the potential of this GRS to predict the plasma TG responsiveness to supplementation with either eicosapentaenoic (EPA) or docosahexaenoic (DHA) acids in the Comparing EPA to DHA (ComparED) Study.
Methods: The ComparED Study is a double-blind, controlled, crossover trial, with participants randomized to three supplemented phases of 10 weeks each: (1) 2.7 g/day of DHA, (2) 2.7 g/day of EPA, and (3) 3 g/day of corn oil (control), separated by 9-week washouts. The 31 SNPs used to build the previous GRS were genotyped in 122 participants of the ComparED Study using TaqMan technology. The GRS for each participant was computed by summing the number of rare alleles. Ordinal and binary logistic models, adjusted for age, sex, and body mass index, were used to calculate the ability of the GRS to predict TG responsiveness.
Results: The GRS predicted TG responsiveness to EPA supplementation (p = 0.006), and a trend was observed for DHA supplementation (p = 0.08). The exclusion of participants with neutral TG responsiveness clarified the association patterns and the predictive capability of the GRS (EPA, p = 0.0003, DHA p = 0.01).
Conclusion: Results of the present study suggest that the constructed GRS is a good predictor of the plasma TG response to supplementation with either DHA or EPA.
Trial registration: ClinicalTrials.gov, NCT01810003. The study protocol was registered on March 4, 2013.
Keywords: DHA; EPA; Genetic risk score; Nutrigenetics; Omega-3 fatty acids; Plasma triglyceride levels.
Conflict of interest statement
BVM and JA received a studentship from the Fonds de recherche du Québec—Santé (FRQS). JA received a studentship from CIHR. JDTM received a postdoctoral fellowship from the FRQS. PC received a scholarship from FRQS. MCV is Tier 1 Canada Research Chair in Genomics Applied to Nutrition and Metabolic Health. Other authors have no conflict of interest to declare.
Figures
References
-
- Binia A, Vargas-Martinez C, Ancira-Moreno M, Gosoniu LM, Montoliu I, Gamez-Valdez E, Soria-Contreras DC, Angeles-Quezada A, Gonzalez-Alberto R, Fernandez S, et al. Improvement of cardiometabolic markers after fish oil intervention in young Mexican adults and the role of PPARalpha L162V and PPARgamma2 P12A. J Nutr Biochem. 2017;43:98–106. doi: 10.1016/j.jnutbio.2017.02.002. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
