

Medical exercise therapy alone versus arthroscopic partial meniscectomy followed by medical exercise therapy for degenerative meniscal tear: a systematic review and meta-analysis of randomized controlled trials
- PMID: 32539864
- PMCID: PMC7296921
- DOI: 10.1186/s13018-020-01741-3
Medical exercise therapy alone versus arthroscopic partial meniscectomy followed by medical exercise therapy for degenerative meniscal tear: a systematic review and meta-analysis of randomized controlled trials
Abstract
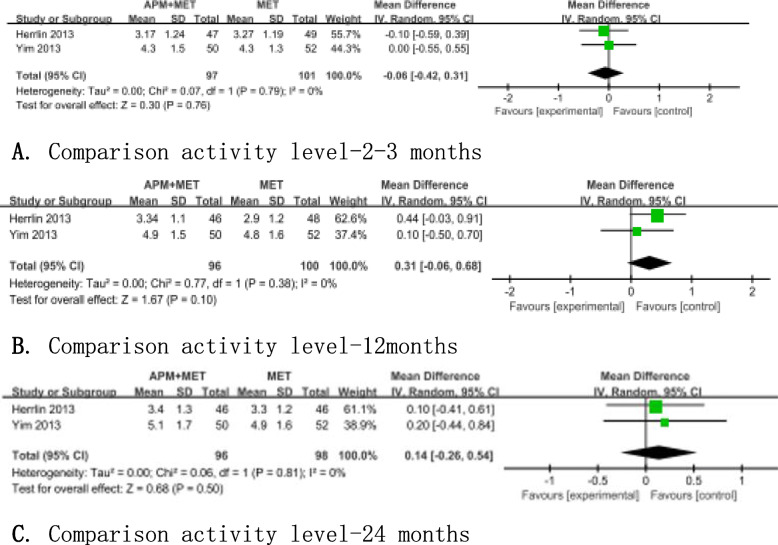
Objective: To explore if medical exercise therapy (MET) alone is comparable to arthroscopic partial meniscectomy (APM) followed by MET for knee pain, activity level, and physical function in middle-aged patients with degenerative meniscal tear (DMT) by a systematic review and meta-analysis of randomized controlled trials (RCTs).
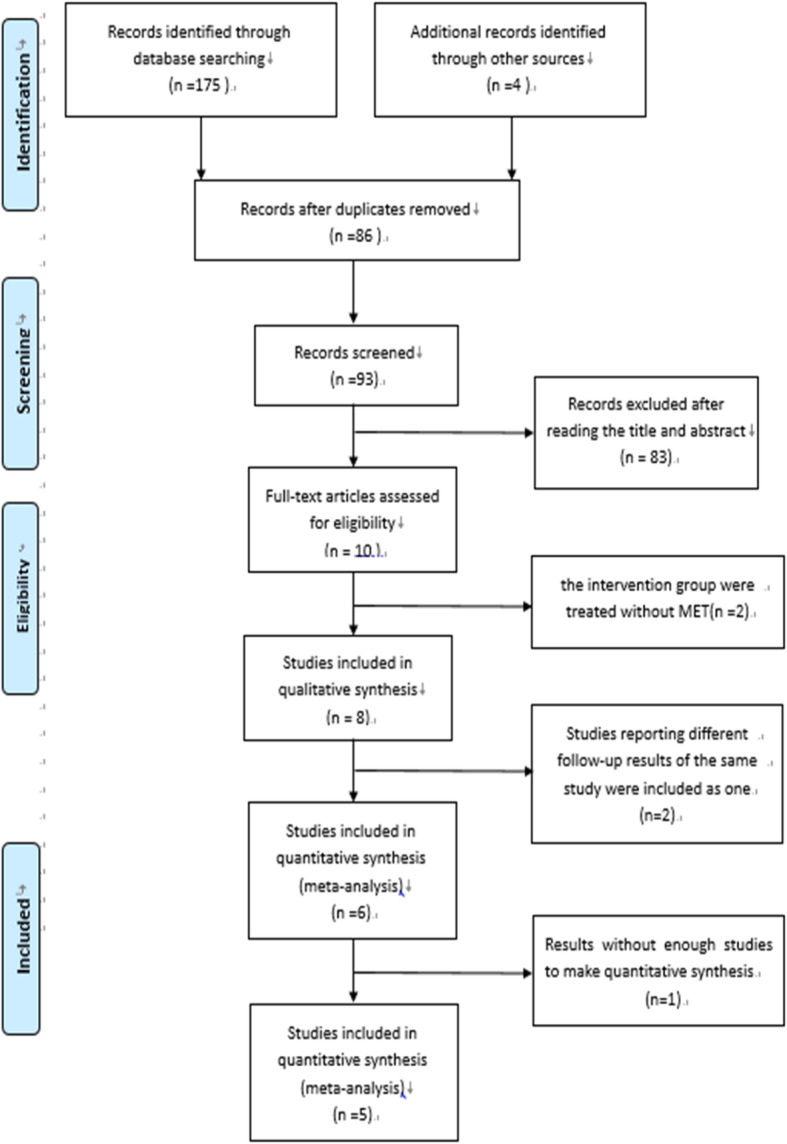
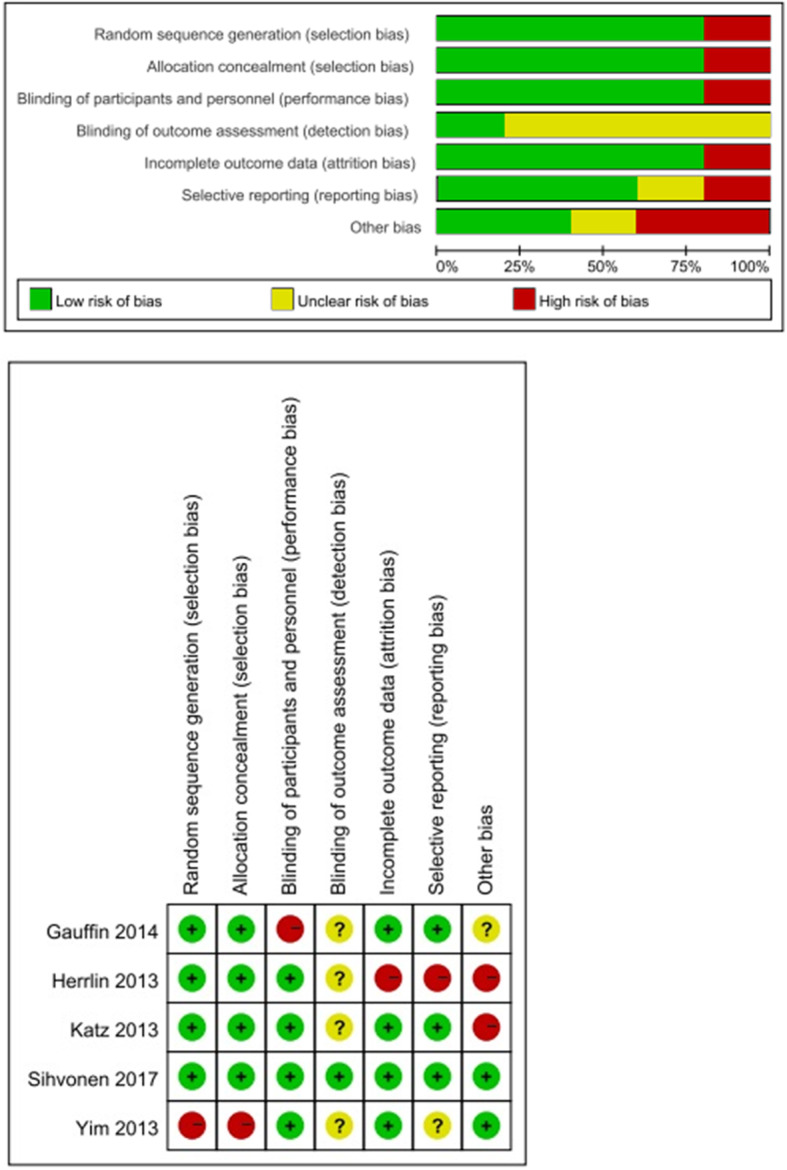
Method: A systematic search of electronic databases (PubMed, the Cochrane Library, Embase, and Web of Science) was conducted to retrieve RCTs comparing MET+APM with MET alone for DMT. Risk of bias of the studies was evaluated. Outcomes assessed were pain relief, physical function, and activity level.
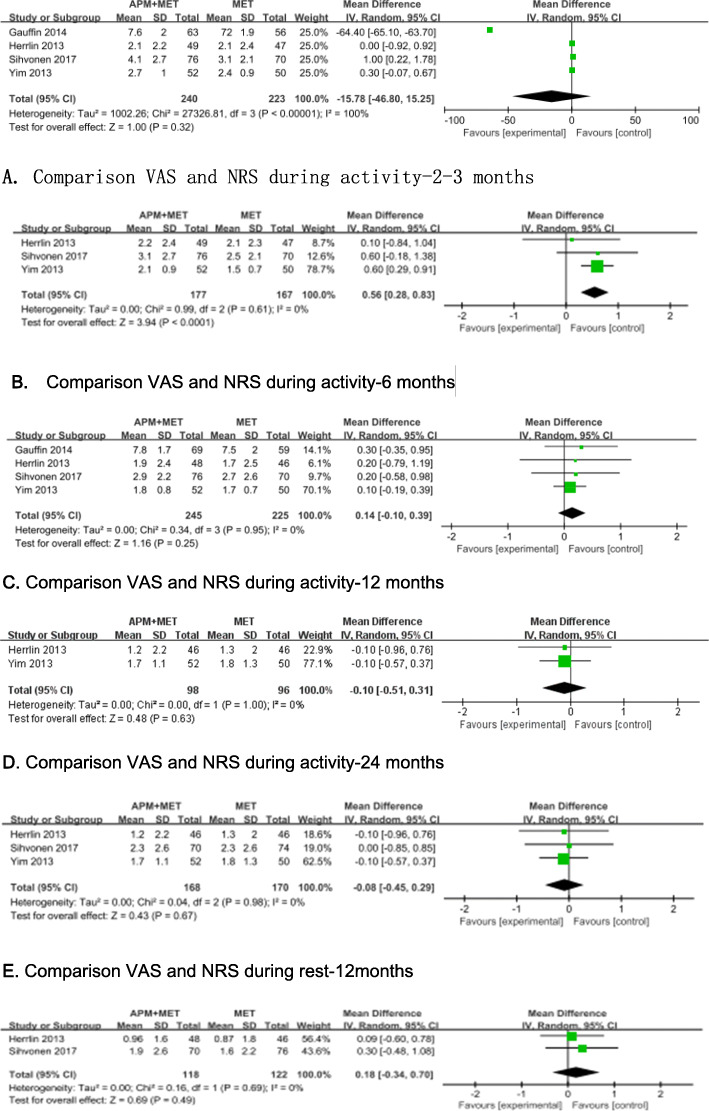
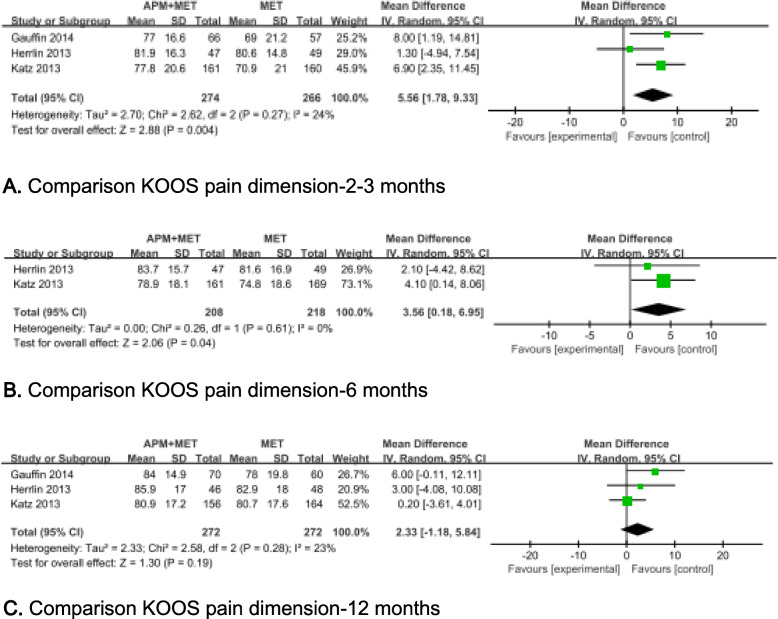
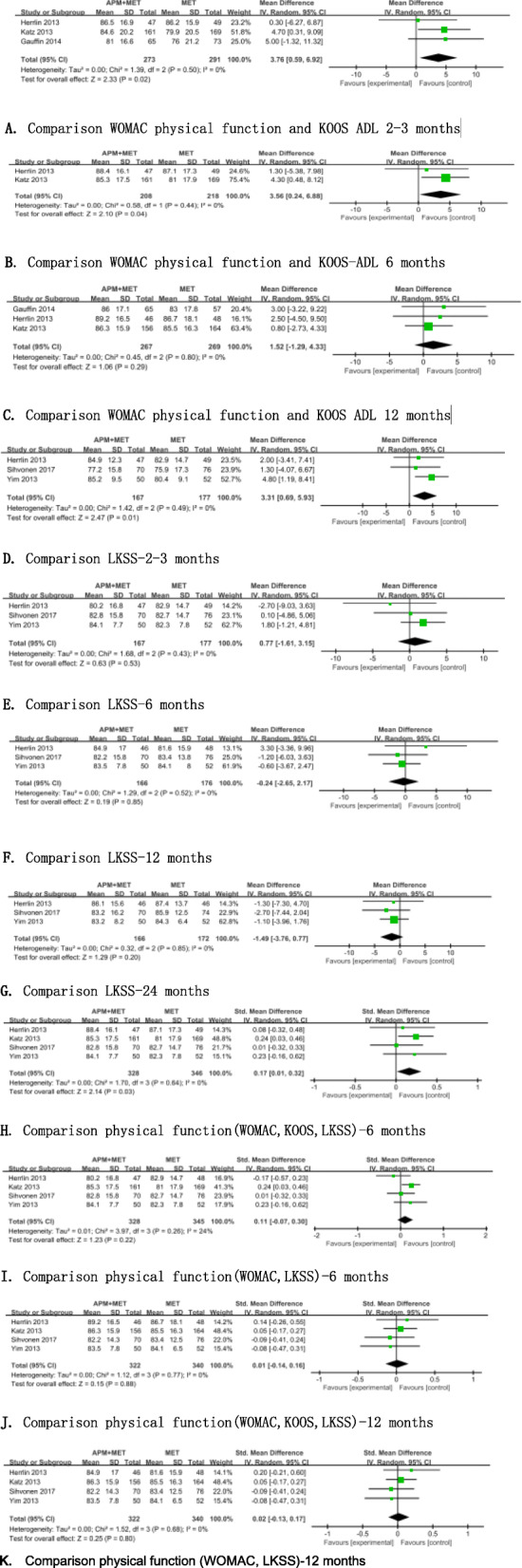
Results: A total of 6 RCTs containing 879 patients were included. After pooling the data of 5 researches, we found small significant differences support the APM + MET group for pain control assessed by Knee injury and Osteoarthritis Outcome Score (KOOS) at 2 to 3 months (p = 0.004) and at 6 months (p = 0.04). And there were statistically improvements in APM + MET at 6 months compared with MET alone when changing measurement to visual analog scale (VAS) (p = 0.0003). Our analysis also found small significant differences favor the APM followed by MET group for physical function both at 2 to 3 months (p = 0.01, KOOS and Western Ontario and McMaster Universities Osteoarthritis Index, WOMAC; and P = 0.40, Lysholm Knee Scoring Scale) and at 6 months (p = 0.01, KOOS and WOMAC).
Conclusion: We found favorable results of APM + MET up to 6 months for pain control and physical function. However, there were no differences at longer follow-up. The clinical applicability of APM + MET compared with MET should be interpreted carefully, and the potential of MET to treat DMT should be valued.
Keywords: Arthroscopic partial meniscectomy; Degenerative meniscal tear; Medical physical therapy; Meta-analysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Aichroth P. Degenerative meniscal tears. Knee. 1994;1:181–182. doi: 10.1016/0968-0160(94)90053-1. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
