

Outcome of robot-assisted pancreaticoduodenectomy during initial learning curve versus laparotomy
- PMID: 32541683
- PMCID: PMC7295787
- DOI: 10.1038/s41598-020-66722-2
Outcome of robot-assisted pancreaticoduodenectomy during initial learning curve versus laparotomy
Abstract
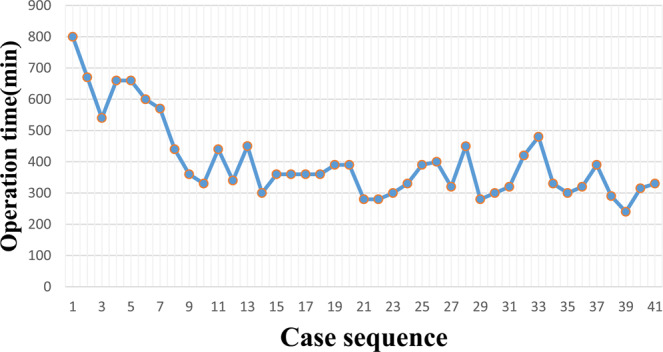
To analyze the initial learning curve (LC) for robot-assisted pancreaticoduodenectomy (RAPD) and compare RAPD during the initial LC with open pancreaticoduodenectomy (OPD) in terms of outcome. This study is a retrospective review of patients who consecutively underwent RAPD and OPD between October 2015 and January 2020 in our hospital. 41 consecutive RAPD cases and 53 consecutive open cases were enrolled for review. Compared with OPD, RAPD required a significantly longer operative time (401.1 ± 127.5 vs. 230.8 ± 44.5 min, P < 0.001) and higher cost (194621 ± 78342 vs. 121874 ± 39973 CNY, P < 0.001). Moreover, compared with the OPD group, the RAPD group revealed a significantly smaller mean number of lymph nodes harvested in malignant cases (15.6 ± 5.9 vs 18.9 ± 7.3, P = 0.025). No statistically significant differences were observed between the two groups in terms of incidence of Clavien-Dindo grade III-V morbidities and 90-day mortality and readmission (P>0.05). In the CUSUM graph, one peak point was observed at the 8th case, after which the operation time began to decrease. LC for RAPD may be less than 30 cases, and RAPD is safe and feasible during the initial LC.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Ielpo, B. et al. Robotic versus standard open pancreatectomy: a propensity score-matched analysis comparison. Updates in surgery, 10.1007/s13304-018-0529-1 (2018). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
