

Prediction of cardiac events using fully automated GLS and BNP titers in patients with known or suspected heart failure
- PMID: 32542005
- PMCID: PMC7295200
- DOI: 10.1371/journal.pone.0234294
Prediction of cardiac events using fully automated GLS and BNP titers in patients with known or suspected heart failure
Abstract
Background: Although global longitudinal strain (GLS) measurements provide useful predictive information, measurement variability is still a major concern. We sought to determine whether fully automated GLS measurements could predict future cardiac events in patients with known or suspected heart failure (HF).
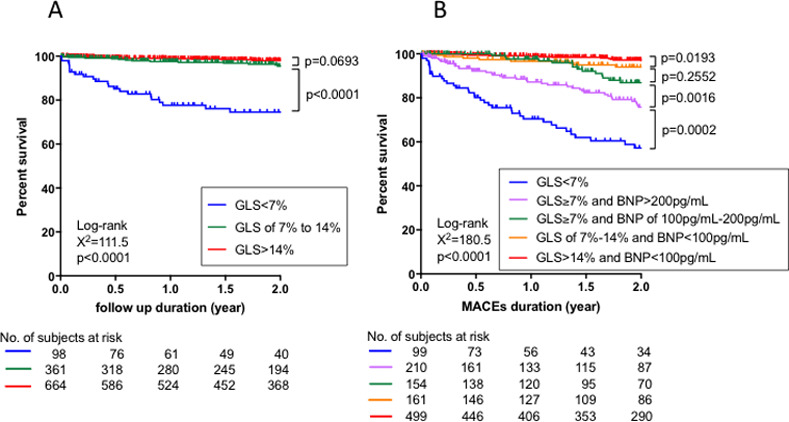
Methods: GLS was measured using fully automated 2D speckle tracking analysis software (AutoStrain, TomTec) in 3,150 subjects who had undergone clinically indicated brain natriuretic peptide (BNP) assays and echocardiographic examinations. Among 1,514 patients in the derivation cohort, optimal cut-off values of BNP and GLS for cardiac death (CD) and major adverse cardiovascular events (MACEs) were determined using survival classification and regression tree (CART) analysis. The remaining 1,636 patients, comprising the validation cohort, were stratified into subgroups according to predefined cut-off values, and survival curves were compared.
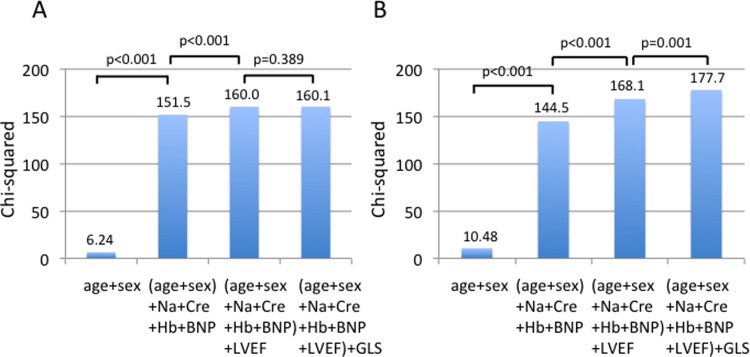
Results: Survival CART analysis selected GLS with cut-off values of 6.2% and 14.0% for predicting CD. GLS of 6.9% and 13.9% and BNP of 83.2 pg/mL and 206.3 pg/mL were selected for predicting MACEs. For simplicity, we defined GLS of 7% and 14% and BNP of 100 pg/mL and 200 pg/mL as cut-off values. These cut-off values stratify high-risk patients in the validation cohort with known or suspected HF for both CD and MACEs.
Conclusions: In addition to BNP, fully automated GLS measurements provide prognostic information for patients with known or suspected HF, and this approach facilitates clinical work flow.
Conflict of interest statement
Dr. Takeuchi has received equipment grant from TomTec. All authors have no other conflicts of interest related to employment, consultancy, patents, products in development, and marketed products. This funding source had no involvement regarding analysis and interpretation of data, writing the manuscript and decision to submit the article for publication. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures



Similar articles
-
A new staging system using right atrial strain in patients with immunoglobulin light-chain cardiac amyloidosis.ESC Heart Fail. 2024 Jun;11(3):1612-1624. doi: 10.1002/ehf2.14710. Epub 2024 Feb 23. ESC Heart Fail. 2024. PMID: 38400613 Free PMC article.
-
Brain natriuretic peptide measurements using standard biochemical equipment: Comparisons with conventional immunoassays.PLoS One. 2022 May 24;17(5):e0268895. doi: 10.1371/journal.pone.0268895. eCollection 2022. PLoS One. 2022. PMID: 35609039 Free PMC article.
-
Feasibility, Reproducibility, and Clinical Implications of the Novel Fully Automated Assessment for Global Longitudinal Strain.J Am Soc Echocardiogr. 2021 Feb;34(2):136-145.e2. doi: 10.1016/j.echo.2020.09.011. Epub 2020 Dec 5. J Am Soc Echocardiogr. 2021. PMID: 33293202
-
B-type natriuretic peptide as a biomarker beyond heart failure: speculations and opportunities.Mayo Clin Proc. 2005 Aug;80(8):1029-36. doi: 10.4065/80.8.1029. Mayo Clin Proc. 2005. PMID: 16092582 Review.
-
[Use of brain natriuretic peptide (BNP) in the diagnosis and treatment of heart failure].Rev Med Suisse Romande. 2003 Feb;123(2):125-8. Rev Med Suisse Romande. 2003. PMID: 15095695 Review. French.
Cited by
-
Cardiac adaptations to patent ductus arteriosus ligation in preterm infants: a speckle-tracking study.Pediatr Res. 2025 Jul 19. doi: 10.1038/s41390-025-04182-y. Online ahead of print. Pediatr Res. 2025. PMID: 40683993
-
Utilizing natriuretic peptides for predicting heart failure risk following myocardial infarction.Cardiovasc Endocrinol Metab. 2025 Jul 15;14(3):e00338. doi: 10.1097/XCE.0000000000000338. eCollection 2025 Sep. Cardiovasc Endocrinol Metab. 2025. PMID: 40672529 Free PMC article.
-
Association Between Indoxyl Sulfate and Dialysis Initiation and Cardiac Outcomes in Chronic Kidney Disease Patients.Int J Nephrol Renovasc Dis. 2022 Mar 26;15:115-126. doi: 10.2147/IJNRD.S354658. eCollection 2022. Int J Nephrol Renovasc Dis. 2022. PMID: 35370416 Free PMC article.
-
Prognostic Value of Right Ventricular Strains Using Novel Three-Dimensional Analytical Software in Patients With Cardiac Disease.Front Cardiovasc Med. 2022 Feb 25;9:837584. doi: 10.3389/fcvm.2022.837584. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35282348 Free PMC article.
-
Left atrioventricular coupling index measured by echocardiography in heart failure with preserved ejection fraction.Sci Rep. 2025 Jul 1;15(1):20419. doi: 10.1038/s41598-025-06291-4. Sci Rep. 2025. PMID: 40594838 Free PMC article.
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. 10.1002/ejhf.592 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
