

The association between use of proton-pump inhibitors and excess mortality after kidney transplantation: A cohort study
- PMID: 32542023
- PMCID: PMC7295199
- DOI: 10.1371/journal.pmed.1003140
The association between use of proton-pump inhibitors and excess mortality after kidney transplantation: A cohort study
Abstract
Background: Chronic use of proton-pump inhibitors (PPIs) is common in kidney transplant recipients (KTRs). However, concerns are emerging about the potential long-term complications of PPI therapy. We aimed to investigate whether PPI use is associated with excess mortality risk in KTRs.
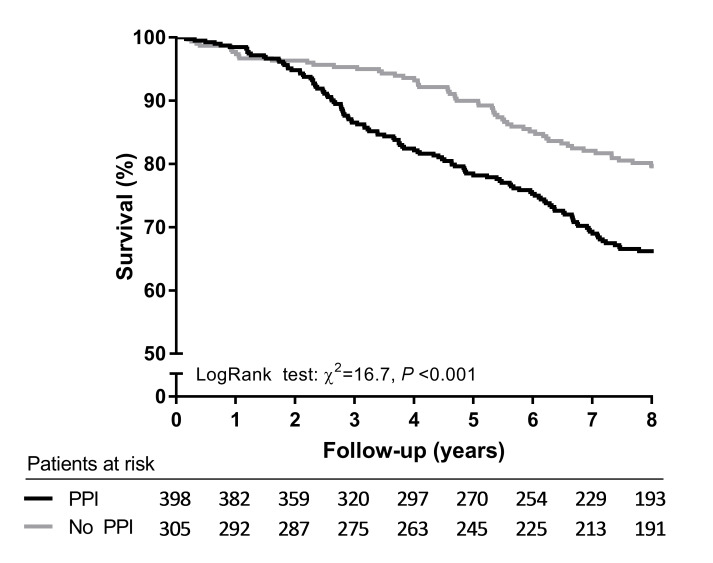
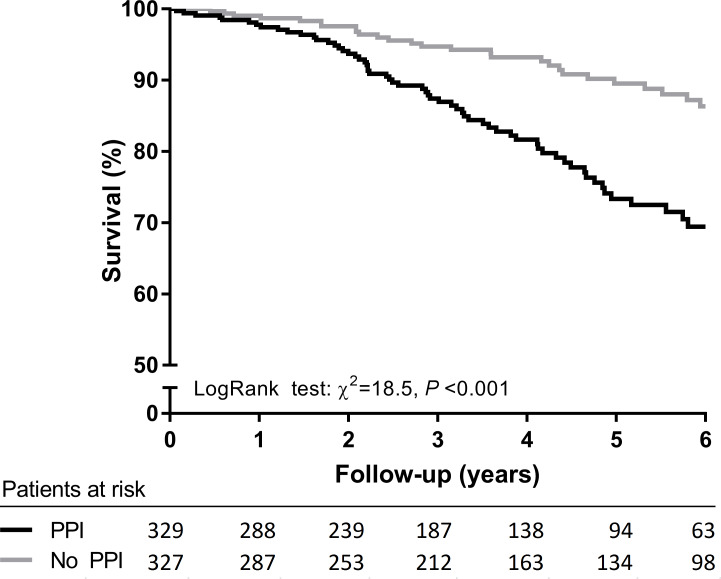
Methods and findings: We investigated the association of PPI use with mortality risk using multivariable Cox proportional hazard regression analyses in a single-center prospective cohort of 703 stable outpatient KTRs, who visited the outpatient clinic of the University Medical Center Groningen (UMCG) between November 2008 and March 2011 (ClinicalTrials.gov Identifier NCT02811835). Independent replication of the results was performed in a prospective cohort of 656 KTRs from the University Hospitals Leuven (NCT01331668). Mean age was 53 ± 13 years, 57% were male, and 56.6% used PPIs. During median follow-up of 8.2 (4.7-9.0) years, 194 KTRs died. In univariable Cox regression analyses, PPI use was associated with an almost 2 times higher mortality risk (hazard ratio [HR] 1.86, 95% CI 1.38-2.52, P < 0.001) compared with no use. After adjustment for potential confounders, PPI use remained independently associated with mortality (HR 1.68, 95% CI 1.21-2.33, P = 0.002). Moreover, the HR for mortality risk in KTRs taking a high PPI dose (>20 mg omeprazole equivalents/day) compared with patients taking no PPIs (HR 2.14, 95% CI 1.48-3.09, P < 0.001) was higher than in KTRs taking a low PPI dose (HR 1.72, 95% CI 1.23-2.39, P = 0.001). These findings were replicated in the Leuven Renal Transplant Cohort. The main limitation of this study is its observational design, which precludes conclusions about causation.
Conclusions: We demonstrated that PPI use is associated with an increased mortality risk in KTRs, independent of potential confounders. Moreover, our data suggest that this risk is highest among KTRs taking high PPI dosages. Because of the observational nature of our data, our results require further corroboration before it can be recommended to avoid the long-term use of PPIs in KTRs.
Trial registration: ClinicalTrials.gov Identifier: NCT02811835, NCT01331668.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999. December;341(23):1725–30. 10.1056/NEJM199912023412303 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
