

Immune suppression in gliomas
- PMID: 32542437
- PMCID: PMC7843555
- DOI: 10.1007/s11060-020-03483-y
Immune suppression in gliomas
Abstract
Introduction: The overall survival in patients with gliomas has not significantly increased in the modern era, despite advances such as immunotherapy. This is in part due to their notorious ability to suppress local and systemic immune responses, severely restricting treatment efficacy.
Methods: We have reviewed the preclinical and clinical evidence for immunosuppression seen throughout the disease process in gliomas. This review aims to discuss the various ways that brain tumors, and gliomas in particular, co-opt the body's immune system to evade detection and ensure tumor survival and proliferation.
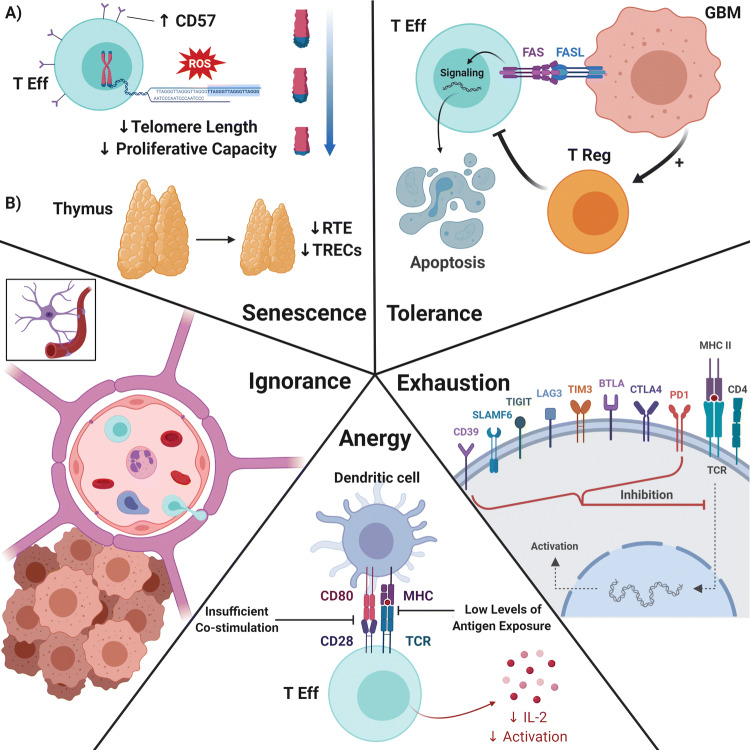
Results: A multitude of mechanisms are discussed by which neoplastic cells evade detection and destruction by the immune system. These include tumor-induced T-cell and NK cell dysfunction, regulatory T-cell and myeloid-derived suppressor cell expansion, M2 phenotypic transformation in glioma-associated macrophages/microglia, upregulation of immunosuppressive glioma cell surface factors and cytokines, tumor microenvironment hypoxia, and iatrogenic sequelae of immunosuppressive treatments.
Conclusions: Gliomas create a profoundly immunosuppressive environment, both locally within the tumor and systemically. Future research should aim to address these immunosuppressive mechanisms in the effort to generate treatment options with meaningful survival benefits for this patient population.
Keywords: Gbm; Glioblastoma; Glioma; Immune suppression; Immunosuppression; Immunotherapy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Dunn GP, Fecci PE, Curry WT (2012) Cancer immunoediting in malignant glioma. Neurosurgery 71:201–22; discussion 222–3. 10.1227/NEU.0b013e31824f840d - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
