

Pseudomonas aeruginosa Strain-sharing in Early Infection Among Children With Cystic Fibrosis
- PMID: 32544950
- PMCID: PMC8563227
- DOI: 10.1093/cid/ciaa788
Pseudomonas aeruginosa Strain-sharing in Early Infection Among Children With Cystic Fibrosis
Abstract
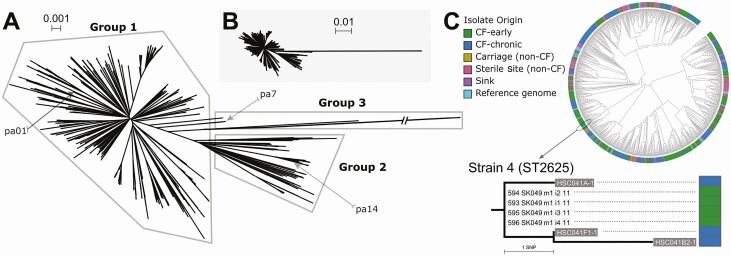
Background: We previously identified Pseudomonas aeruginosa isolates with characteristics typical of chronic infection in some early infections in children with cystic fibrosis (CF), suggesting that these isolates may have been acquired from other patients. Our objective was to define the extent of P. aeruginosa strain-sharing in early CF infections and its impact on antibiotic eradication treatment failure rates.
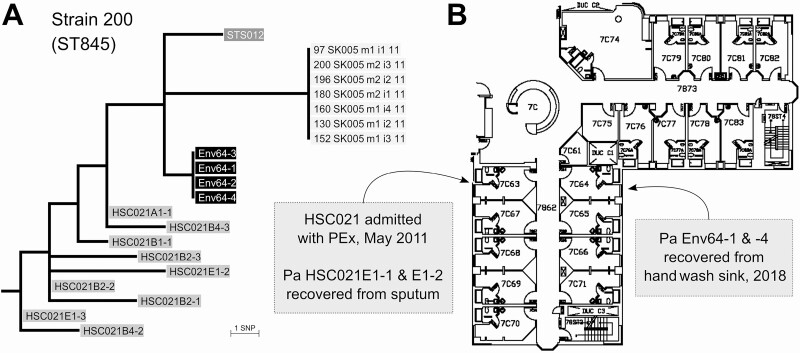
Methods: We performed whole genome sequencing on isolates from early pediatric CF pulmonary infections and from the following comparator groups in the same hospital: chronic CF infection, sink drains, sterile site infections, and asymptomatic carriage. Univariate logistic regression was used to assess factors associated with treatment failure.
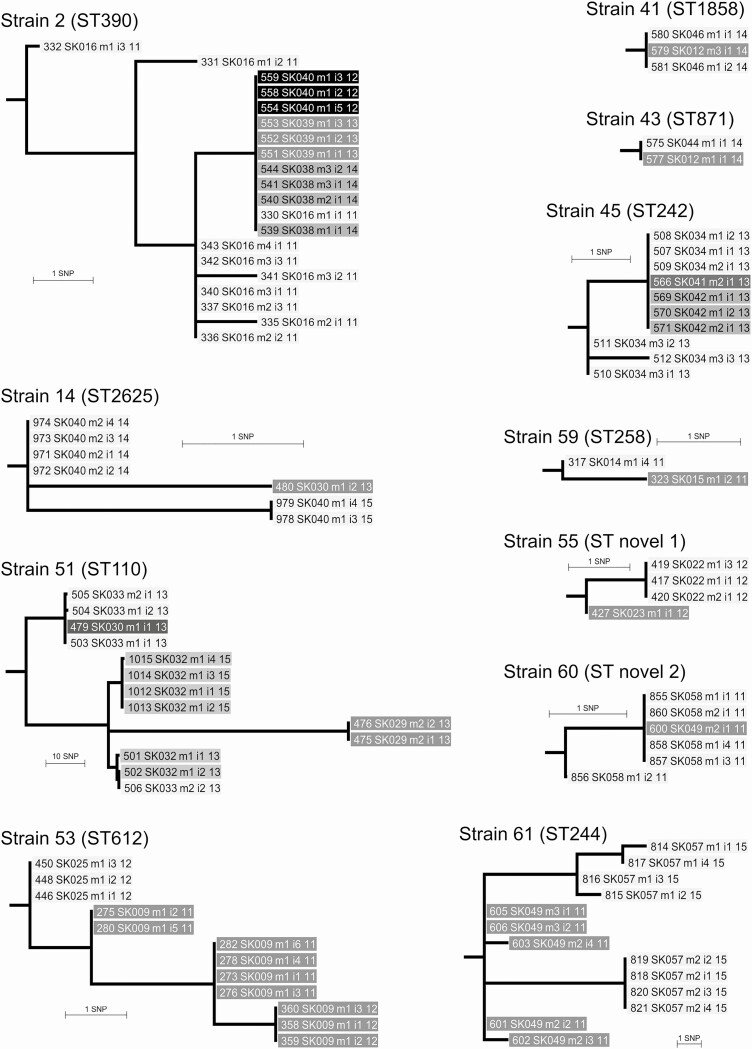
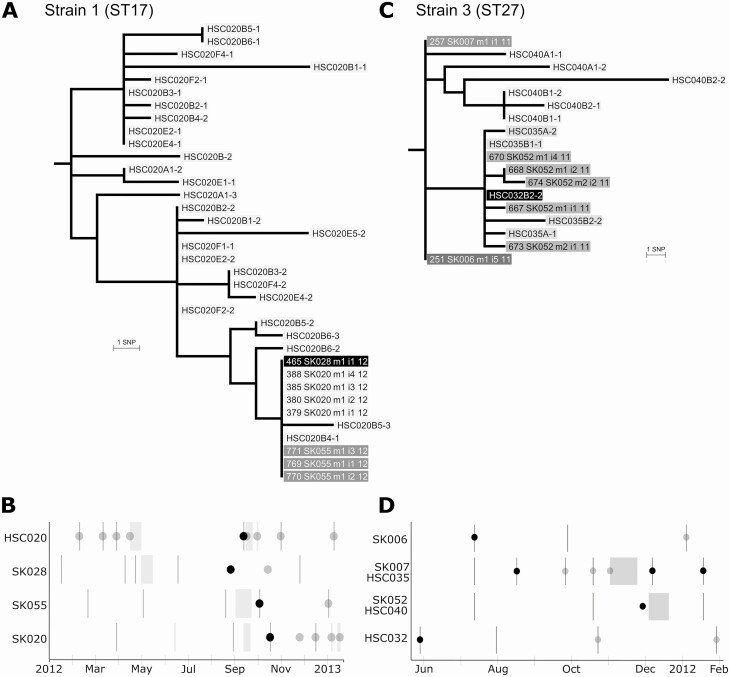
Results: In this retrospective, observational study, 1029 isolates were sequenced. The CF clones strain B and clone C were present. In 70 CF patients with early infections, 14 shared strains infected 29 (41%) patients over 5 years; 16% (n = 14) of infections had mixed strains. In the 70 children, approximately one-third of shared-strain infections were likely due to patient-to-patient transmission. Mixed-strain infections were associated with strain-sharing (odds ratio, 8.50; 95% confidence interval, 2.2-33.4; P = .002). Strain-sharing was not associated with antibiotic eradication treatment failure; however, nosocomial strain transmission was associated with establishment of chronic infection in a CF sibling pair.
Conclusions: Although early P. aeruginosa CF infection is thought to reflect acquisition of diverse strains from community reservoirs, we identified frequent early CF strain-sharing that was associated with the presence of mixed strains and instances of possible patient-to-patient transmission.
Keywords: Pseudomonas aeruginosa; cross infection; cystic fibrosis; respiratory tract infections; whole genome sequencing.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Pseudomonas aeruginosa and Children With Cystic Fibrosis.Clin Infect Dis. 2021 Nov 2;73(9):e2529-e2530. doi: 10.1093/cid/ciaa765. Clin Infect Dis. 2021. PMID: 32544945 No abstract available.
References
-
- Ranganathan SC, Skoric B, Ramsay KA, et al. ; Australian Respiratory Early Surveillance Team for Cystic Fibrosis . Geographical differences in first acquisition of Pseudomonas aeruginosa in cystic fibrosis. Ann Am Thorac Soc 2013; 10:108–14. - PubMed
-
- Hogardt M, Heesemann J. Adaptation of Pseudomonas aeruginosa during persistence in the cystic fibrosis lung. Int J Med Microbiol 2010; 300:557–62. - PubMed
-
- Vidya P, Smith L, Beaudoin T, et al. Chronic infection phenotypes of Pseudomonas aeruginosa are associated with failure of eradication in children with cystic fibrosis. Eur J Clin Microbiol Infect Dis 2016; 35:67–74. - PubMed
-
- Kidd TJ, Ramsay KA, Vidmar S, et al. ; ACFBAL Study Investigators . Pseudomonas aeruginosa genotypes acquired by children with cystic fibrosis by age 5-years. J Cyst Fibros 2015; 14:361–9. - PubMed
