

Modern Radiotherapy for Pediatric Brain Tumors
- PMID: 32545204
- PMCID: PMC7352417
- DOI: 10.3390/cancers12061533
Modern Radiotherapy for Pediatric Brain Tumors
Abstract
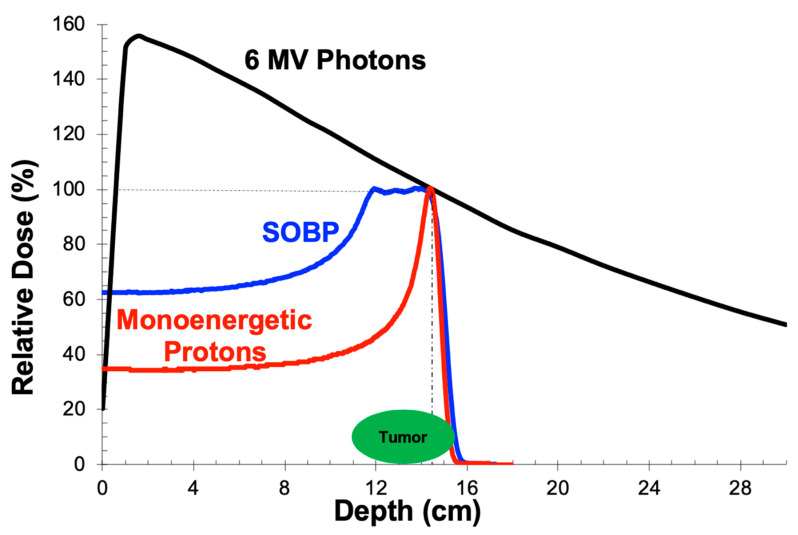
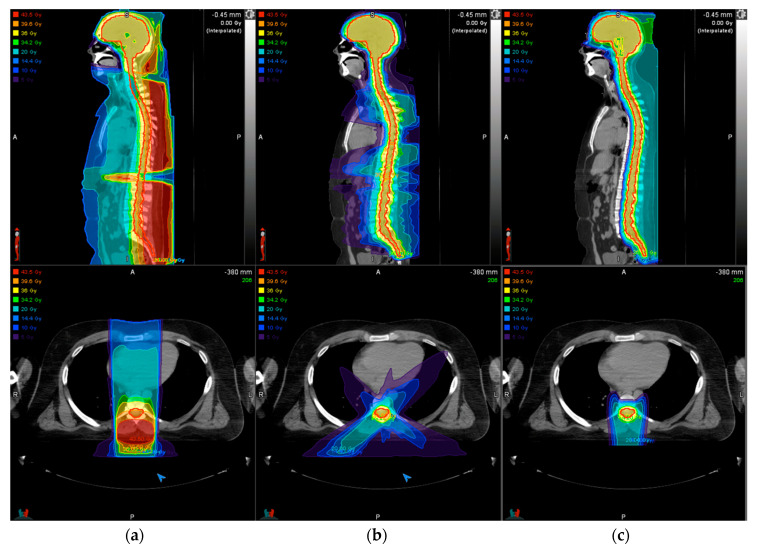
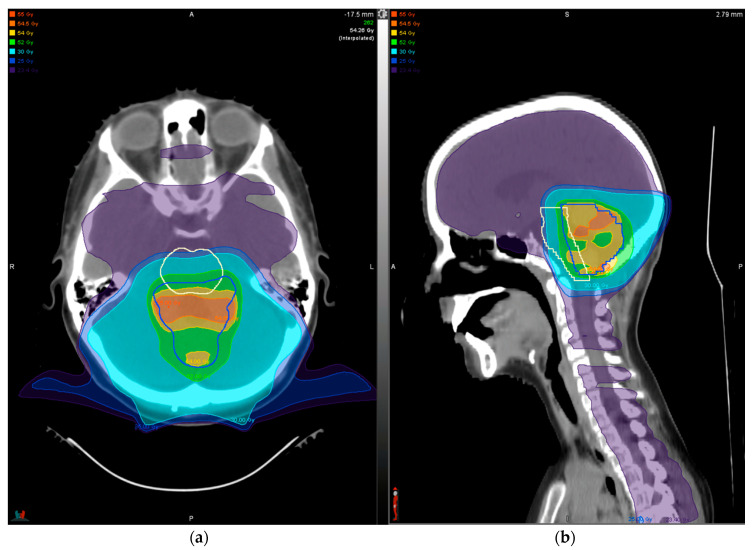
Cancer is a leading cause of death in children with tumors of the central nervous system, the most commonly encountered solid malignancies in this population. Radiotherapy (RT) is an integral part of managing brain tumors, with excellent long-term survival overall. The tumor histology will dictate the volume of tissue requiring treatment and the dose. However, radiation in developing children can yield functional deficits and/or cosmetic defects and carries a risk of second tumors. In particular, children receiving RT are at risk for neurocognitive effects, neuroendocrine dysfunction, hearing loss, vascular anomalies and events, and psychosocial dysfunction. The risk of these late effects is directly correlated with the volume of tissue irradiated and dose delivered and is inversely correlated with age. To limit the risk of developing these late effects, improved conformity of radiation to the target volume has come from adopting a volumetric planning process. Radiation beam characteristics have also evolved to achieve this end, as exemplified through development of intensity modulated photons and the use of protons. Understanding dose limits of critical at-risk structures for different RT modalities is evolving. In this review, we discuss the physical basis of the most common RT modalities used to treat pediatric brain tumors (intensity modulated radiation therapy and proton therapy), the RT planning process, survival outcomes for several common pediatric malignant brain tumor histologies, RT-associated toxicities, and steps taken to mitigate the risk of acute and late effects from treatment.
Keywords: IMRT; childhood; late effects; pediatric brain tumors; proton; radiation; radiotherapy; survival; toxicity; treatment planning.
Conflict of interest statement
N.J.D. declares no relevant conflicts of interest. T.I.Y. declares in-kind support from MIM software for the PPCR.
Figures
References
-
- Howlader N.N.A., Noone A.M., Krapcho M., Miller D., Brest A., Yu M., Ruhl J., Tatalovich Z., Mariotto A., Lewis D.R., et al. SEER Cancer Statistics Review, 1975–2016. National Cancer Institute; Bethesda, MD, USA: 2019. https://seer.cancer.gov/csr/1975_2016/ , based on November 2018 SEER data submission, posted to the SEER web site, April 2019.
-
- Merchant T.E., Conklin H.M., Wu S., Lustig R.H., Xiong X. Late effects of conformal radiation therapy for pediatric patients with low-grade glioma: Prospective evaluation of cognitive, endocrine, and hearing deficits. J. Clin. Oncol. 2009;27:3691–3697. doi: 10.1200/JCO.2008.21.2738. - DOI - PMC - PubMed
-
- Paulino A.C., Lobo M., Teh B.S., Okcu M.F., South M., Butler E.B., Su J., Chintagumpala M. Ototoxicity after intensity-modulated radiation therapy and cisplatin-based chemotherapy in children with medulloblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2010;78:1445–1450. doi: 10.1016/j.ijrobp.2009.09.031. - DOI - PubMed
-
- Vatner R.E., Niemierko A., Misra M., Weyman E.A., Goebel C.P., Ebb D.H., Jones R.M., Huang M.S., Mahajan A., Grosshans D.R., et al. Endocrine Deficiency As a Function of Radiation Dose to the Hypothalamus and Pituitary in Pediatric and Young Adult Patients With Brain Tumors. J. Clin. Oncol. 2018;36:2854–2862. doi: 10.1200/JCO.2018.78.1492. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
