

Carotid Intima-Media Thickness Progression as Surrogate Marker for Cardiovascular Risk: Meta-Analysis of 119 Clinical Trials Involving 100 667 Patients
- PMID: 32546049
- PMCID: PMC7115957
- DOI: 10.1161/CIRCULATIONAHA.120.046361
Carotid Intima-Media Thickness Progression as Surrogate Marker for Cardiovascular Risk: Meta-Analysis of 119 Clinical Trials Involving 100 667 Patients
Abstract
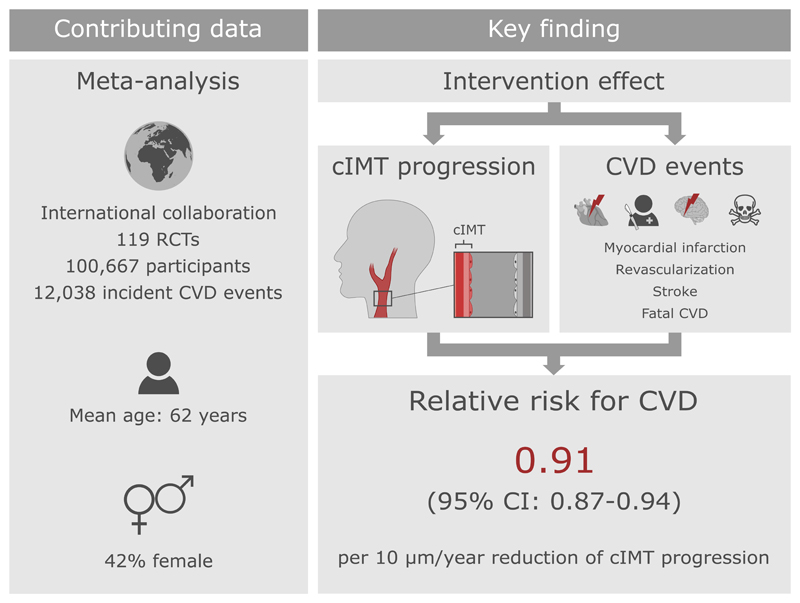
Background: To quantify the association between effects of interventions on carotid intima-media thickness (cIMT) progression and their effects on cardiovascular disease (CVD) risk.
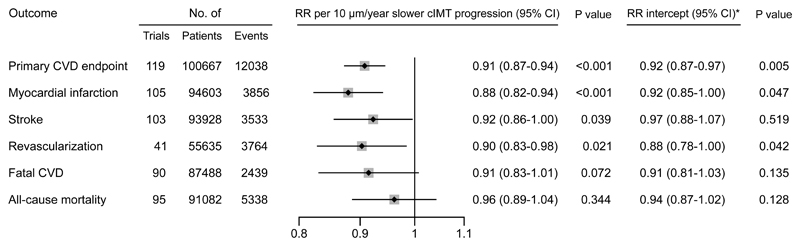
Methods: We systematically collated data from randomized, controlled trials. cIMT was assessed as the mean value at the common-carotid-artery; if unavailable, the maximum value at the common-carotid-artery or other cIMT measures were used. The primary outcome was a combined CVD end point defined as myocardial infarction, stroke, revascularization procedures, or fatal CVD. We estimated intervention effects on cIMT progression and incident CVD for each trial, before relating the 2 using a Bayesian meta-regression approach.
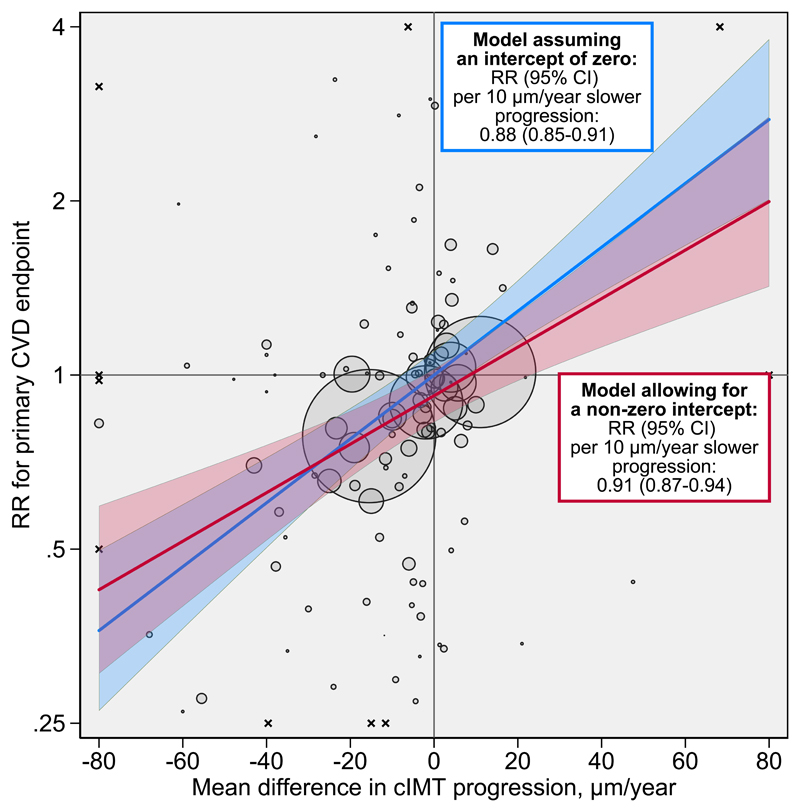
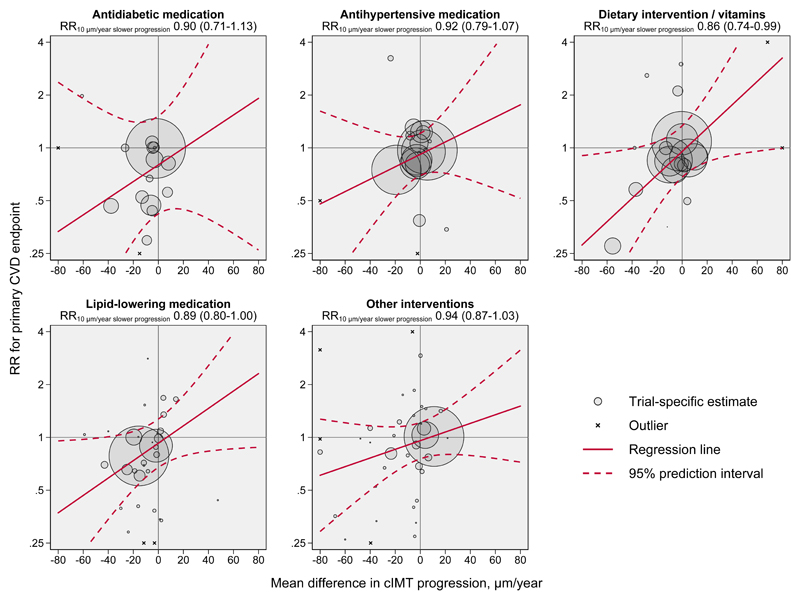
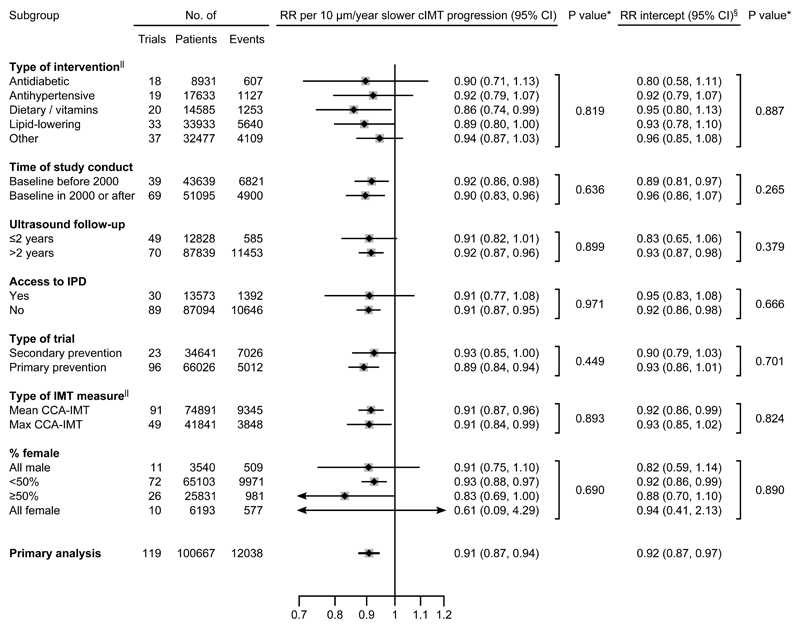
Results: We analyzed data of 119 randomized, controlled trials involving 100 667 patients (mean age 62 years, 42% female). Over an average follow-up of 3.7 years, 12 038 patients developed the combined CVD end point. Across all interventions, each 10 μm/y reduction of cIMT progression resulted in a relative risk for CVD of 0.91 (95% Credible Interval, 0.87-0.94), with an additional relative risk for CVD of 0.92 (0.87-0.97) being achieved independent of cIMT progression. Taken together, we estimated that interventions reducing cIMT progression by 10, 20, 30, or 40 μm/y would yield relative risks of 0.84 (0.75-0.93), 0.76 (0.67-0.85), 0.69 (0.59-0.79), or 0.63 (0.52-0.74), respectively. Results were similar when grouping trials by type of intervention, time of conduct, time to ultrasound follow-up, availability of individual-participant data, primary versus secondary prevention trials, type of cIMT measurement, and proportion of female patients.
Conclusions: The extent of intervention effects on cIMT progression predicted the degree of CVD risk reduction. This provides a missing link supporting the usefulness of cIMT progression as a surrogate marker for CVD risk in clinical trials.
Keywords: cardiovascular disease; carotid intima-media thickness; clinical trials as topic; meta-analysis; surrogate marker.
Conflict of interest statement
P. Willeit reports grants from the German Research Foundation DFG, the Austrian Science Fund FWF, the Austrian Research Promotion Agency FFG and the Dr.-Johannes-and-Hertha-Tuba Foundation during the conduct of the study. L. Tschiderer reports grants from the Dr.-Johannes-and-Hertha-Tuba Foundation during the conduct of the study and non-financial support from Sanofi outside the submitted work. E. Allara was supported by a National Institute for Health Research PhD studentship (NIHR BTRU-2014-10024) during the conduction of this study and reports support from EU/EFPIA Innovative Medicines Initiative Joint Undertaking BigData@Heart grant n° 116074 outside the submitted work. L. Seekircher reports non-financial support from Sanofi outside the submitted work. H.C. Gerstein reports grants from Sanofi, Eli Lilly, Astra Zeneca, Boehringer Ingelheim, Novo Nordisk, Merck, and Abbott, and personal fees from Sanofi, Eli Lilly, Astra Zeneca, Boehringer Ingelheim, Abbott, Novo Nordisk, Merck, Jannsen, Kowa Research Institute, and Cirius outside the submitted work. E. Stroes reports Lecturing/ad-boards fees paid to institution by Amgen, Sanofi-Regeneron, Novartis, Athera, Mylan unrelated to the present work. K. Kapellas reports grants from the National Health and Medical Research Council during the conduct of the study. M. Skilton reports grants from the National Health and Medical Research Council of Australia during the conduct of the study. M.G.A. van Vonderen reports grants from Abbott International and Boehringer Ingelheim during the conduct of the study. S. Kiechl reports grants from the Austrian Promotion Agency FFG outside the submitted work. G. Klingenschmid reports non-financial support from Sanofi and Pfizer outside the submitted work. S.E. Kjeldsen reports personal fees from Bayer, Merck KGaA, MSD, Sanofi, and Takeda outside the submitted work. M.H. Olsen reports grants from the Novo Nordic Foundation outside the submitted work. N. Sattar reports personal fees from Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, NAPP Pharmaceuticals, Novo Nordisk, and Sanofi, and grants from Boehringer Ingelheim outside the submitted work. M.P.C. Grooteman reports grants from the Dutch Kidney Foundation, Fresenius Medical Care Netherlands BV, Gambro Sweden, the Twiss Fund, and ZON MW during the conduct of the study. P.J. Blankestijn reports grants from the European Commission and other financial activities from Medtronic, Baxter, and Braun outside the submitted work. M.L. Bots reports grants from AstraZeneca outside the submitted work. M.J. Sweeting reports grants from the German Research Foundation during the conduct of the study. S.G. Thompson reports grants from the UK Medical Research Council, the British Heart Foundation, and the German Research Foundation DFG during the conduct of the study. M.W. Lorenz reports grants from the German Research Foundation DFG during the conduct of the study. Other authors have no conflicts of interests.
Figures
Comment in
-
Does Reduced Carotid Intima Media Thickness Progression Predict Cardiovascular Risk Reduction?Circulation. 2020 Aug 18;142(7):643-644. doi: 10.1161/CIRCULATIONAHA.120.048890. Epub 2020 Aug 17. Circulation. 2020. PMID: 32804564 No abstract available.
References
-
- Lorenz MW, Polak JF, Kavousi M, Mathiesen EB, Völzke H, Tuomainen T-P, Sander D, Plichart M, Catapano AL, Robertson CM, et al. Carotid intima-media thickness progression to predict cardiovascular events in the general population (the PROG-IMT collaborative project): a meta-analysis of individual participant data. Lancet. 2012;379:2053–2062. doi: 10.1016/S0140-6736(12)60441-3. - DOI - PMC - PubMed
-
- Willeit P, Thompson SG, Agewall S, Bergström G, Bickel H, Catapano AL, Chien K-L, de Groot E, Empana J-P, Etgen T, et al. Inflammatory markers and extent and progression of early atherosclerosis: Meta-analysis of individual-participant-data from 20 prospective studies of the PROG-IMT collaboration. Eur J Cardiovasc Prev Rehabil. 2016;23:194–205. doi: 10.1177/2047487314560664. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
