

Newborn screening alone insufficient to improve pulmonary outcomes for cystic fibrosis
- PMID: 32546430
- PMCID: PMC7736297
- DOI: 10.1016/j.jcf.2020.06.002
Newborn screening alone insufficient to improve pulmonary outcomes for cystic fibrosis
Abstract
Background: The Wisconsin Cystic Fibrosis Neonatal Screening Project was a randomized clinical trial (RCT) revealing that children receiving an early diagnosis of CF via newborn screening (NBS) had improved nutritional outcomes but similar lung disease severity compared to those who presented clinically. Because the evaluations of these subjects by protocol ended in 2012, our objective was to assess long-term pulmonary and mortality outcomes.
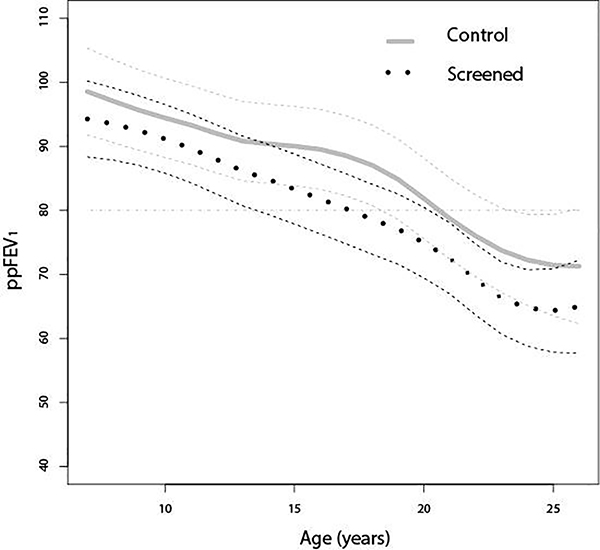
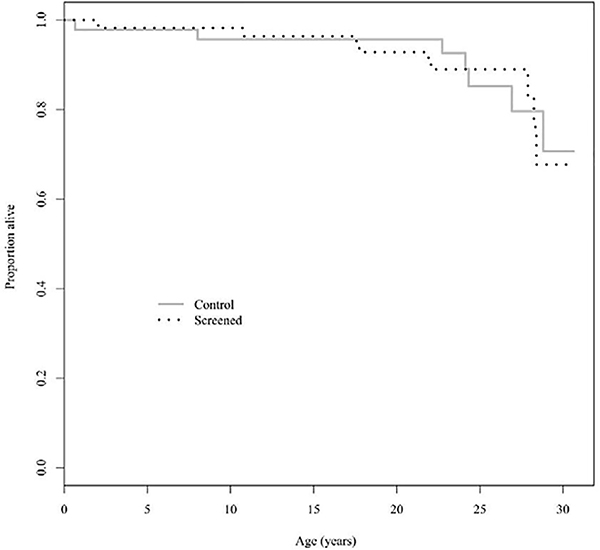
Methods: Retrospective analysis of the RCT cohort utilized longitudinal outcome measures obtained from the Cystic Fibrosis Foundation Patient Registry (CFFPR). Data included screening assignment, clinical characteristics, percent predicted forced expiratory volume in 1 s (ppFEV1) and mortality. A random intercept model was used to compare the ppFEV1 decline of subjects between the two groups up to age 26 years. Mortality was analyzed using the Kaplan-Meier method.
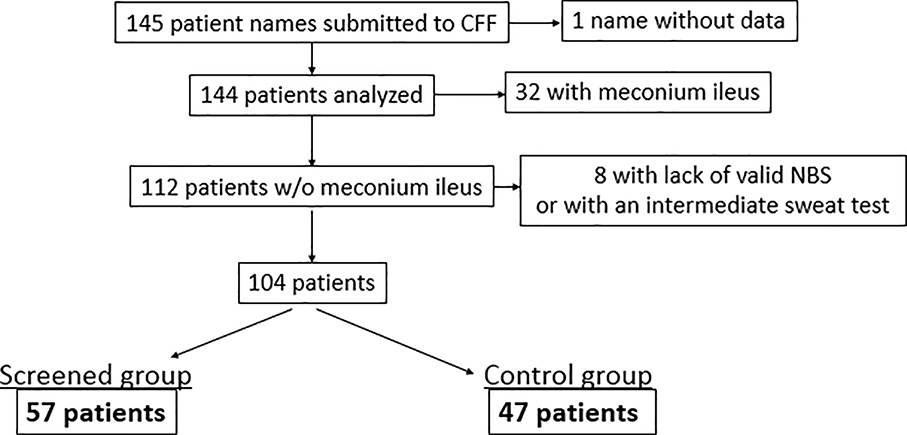
Results: Of the 145 subjects who consented to the original study, 104 subjects met inclusion criteria and had adequate data in the CFFPR. Of 57 subjects in the screened group and 47 in the control group, the rates of ppFEV1 decline were 1.76%/year (95% CI 1.62 to 1.91%) and 1.43%/year (95% CI 1.26 to 1.60%), respectively (p<0.0002). Pseudomonas aeruginosa acquired before 2 years was partially responsible. There was no difference in mortality between the two groups.
Conclusions: NBS alone does not improve pulmonary outcomes in CF, particularly when other risk factors supervene. In an era prior to strict infection control and current therapies, NBS for CF may be associated with worse pulmonary outcomes.
Keywords: Cystic fibrosis; Forced expiratory volume; Mortality; Newborn screening; Phenotype; Pseudomonas aeruginosa.
Copyright © 2020. Published by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest The authors have no conflicts of interest relevant to this article to disclose.
Figures
References
-
- Farrell PM, Kosorok MR, Rock MJ, Laxova A, Zeng L, Lai H, et al. Early diagnosis of cystic fibrosis through neonatal screening prevents severe malnutrition and improves long-term growth. Pediatrics 2001;107(1):1–13. - PubMed
-
- Grosse SD, Rosenfeld M, Devine OJ, Lai H, Farrell PM. Potential impact of newborn screening for cystic fibrosis on child survival: A systematic review and analysis. J Pediatr. 2006;149(3):362–6. - PubMed
-
- Castellani C Evidence for newborn screening for cystic fibrosis. Paediatr Respir Rev. 2003;4(4):278–84. - PubMed
-
- Dijk FN, McKay K, Barzi F, Gaskin KJ, Fitzgerald DA. Improved survival in cystic fibrosis patients diagnosed by newborn screening compared to a historical cohort from the same centre. Arch Dis Child. 2011;96(12):1118–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
