

Management of adults with coarctation of aorta
- PMID: 32547712
- PMCID: PMC7284000
- DOI: 10.4330/wjc.v12.i5.167
Management of adults with coarctation of aorta
Abstract
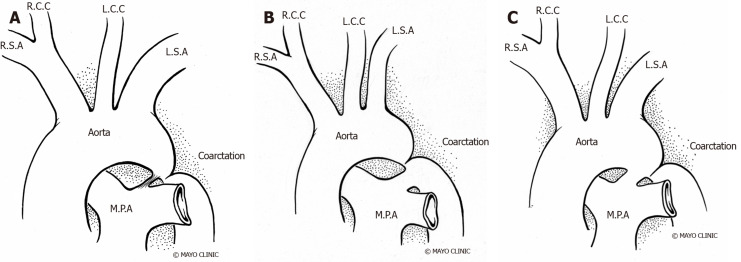
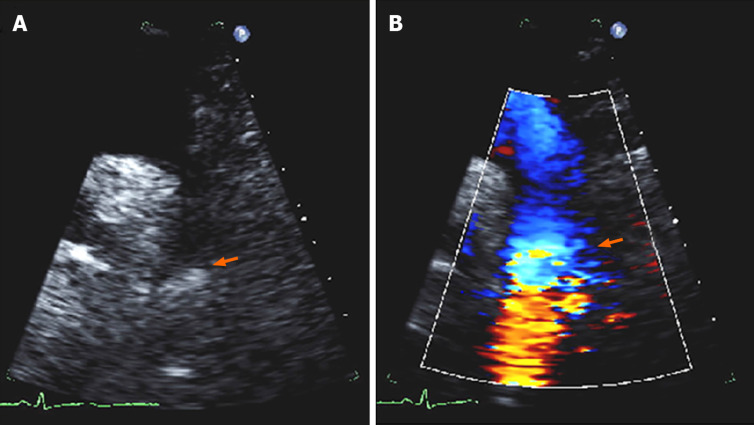
Coarctation of the aorta (CoA) is a relatively common congenital cardiac defect often causing few symptoms and therefore can be challenging to diagnose. The hallmark finding on physical examination is upper extremity hypertension, and for this reason, CoA should be considered in any young hypertensive patient, justifying measurement of lower extremity blood pressure at least once in these individuals. The presence of a significant pressure gradient between the arms and legs is highly suggestive of the diagnosis. Early diagnosis and treatment are important as long-term data consistently demonstrate that patients with CoA have a reduced life expectancy and increased risk of cardiovascular complications. Surgical repair has traditionally been the mainstay of therapy for correction, although advances in endovascular technology with covered stents or stent grafts permit nonsurgical approaches for the management of older children and adults with native CoA and complications. Persistent hypertension and vascular dysfunction can lead to an increased risk of coronary disease, which, remains the greatest cause of long-term mortality. Thus, blood pressure control and periodic reassessment with transthoracic echocardiography and three-dimensional imaging (computed tomography or cardiac magnetic resonance) for should be performed regularly as cardiovascular complications may occur decades after the intervention.
Keywords: Balloon angioplasty; Cardiac catheterization; Cardiac surgery; Coarctation of aorta; Stents.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures






Similar articles
-
Blood Pressure Behavior After Correction Adult Coarctation of Aorta Short Term Follows Up.Med Arch. 2021 Aug;75(4):269-273. doi: 10.5455/medarh.2021.75.269-273. Med Arch. 2021. PMID: 34759446 Free PMC article.
-
Coarctation of Aorta in Children.Cureus. 2018 Dec 5;10(12):e3690. doi: 10.7759/cureus.3690. Cureus. 2018. PMID: 30761242 Free PMC article. Review.
-
Acute outcome of stent therapy for coarctation of the aorta: results of the coarctation of the aorta stent trial.Catheter Cardiovasc Interv. 2013 Oct 1;82(4):503-10. doi: 10.1002/ccd.24949. Epub 2013 May 15. Catheter Cardiovasc Interv. 2013. PMID: 23592408 Clinical Trial.
-
Endovascular stents for coarctation of the aorta: initial results and intermediate-term follow-up.J Am Coll Cardiol. 2001 Nov 1;38(5):1518-23. doi: 10.1016/s0735-1097(01)01572-8. J Am Coll Cardiol. 2001. PMID: 11691533
-
Diagnosis, imaging and clinical management of aortic coarctation.Heart. 2017 Aug;103(15):1148-1155. doi: 10.1136/heartjnl-2017-311173. Epub 2017 Apr 4. Heart. 2017. PMID: 28377475 Review.
Cited by
-
An in silico analysis of heart rate impact on wall shear stress hemodynamic parameters in aortic coarctation.Sci Rep. 2025 Jan 22;15(1):2747. doi: 10.1038/s41598-025-85522-0. Sci Rep. 2025. PMID: 39837894 Free PMC article.
-
Consistency of the continuous flow pressure gradient despite aortic arch anomalies co-existing with coarctation.medRxiv [Preprint]. 2023 Oct 30:2023.10.30.23297763. doi: 10.1101/2023.10.30.23297763. medRxiv. 2023. PMID: 37961134 Free PMC article. Preprint.
-
End-to-side anastomosis and autologous pulmonary artery patch for aortic coarctation and hypoplastic aortic arch.J Thorac Dis. 2025 Feb 28;17(2):959-968. doi: 10.21037/jtd-24-1635. Epub 2025 Feb 27. J Thorac Dis. 2025. PMID: 40083496 Free PMC article.
-
Mini-access ascending aorto-bifemoral bypass surgery for the treatment of aortic steno-occlusive disease.JTCVS Tech. 2024 Jan 19;24:14-19. doi: 10.1016/j.xjtc.2024.01.006. eCollection 2024 Apr. JTCVS Tech. 2024. PMID: 38835566 Free PMC article.
-
Select Congenital Heart Disease: Important Echocardiographic Features and Changes during Pregnancy.Rev Cardiovasc Med. 2023 Feb 22;24(3):66. doi: 10.31083/j.rcm2403066. eCollection 2023 Mar. Rev Cardiovasc Med. 2023. PMID: 39077484 Free PMC article. Review.
References
-
- Salahuddin A, Chan a, Zaidi AN. The Adult with Coarctation of the Aorta. Congenital Heart Disease. 2018
-
- Thiene G. [G. B. Morgagni: De sedibus et causis morborum per anatomen indagatis] G Ital Cardiol. 1985;15:558–560. - PubMed
-
- Grech V. Diagnostic and surgical trends, and epidemiology of coarctation of the aorta in a population-based study. Int J Cardiol. 1999;68:197–202. - PubMed
-
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–1900. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
