

Current therapy of KRAS-mutant lung cancer
- PMID: 32548736
- PMCID: PMC7680319
- DOI: 10.1007/s10555-020-09903-9
Current therapy of KRAS-mutant lung cancer
Abstract
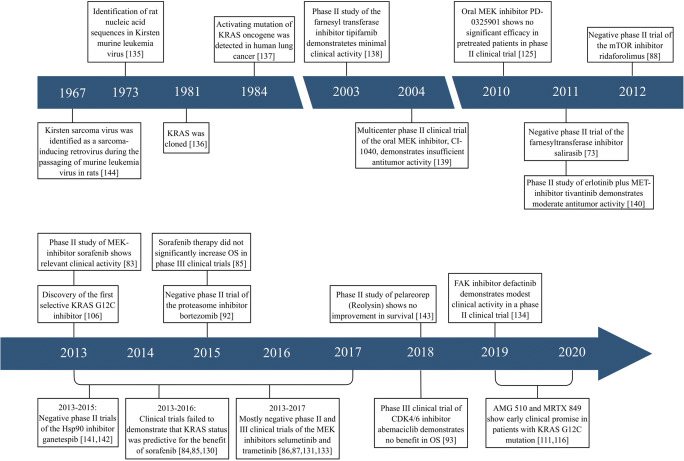
KRAS mutations are the most frequent gain-of-function alterations in patients with lung adenocarcinoma (LADC) in the Western world. Although they have been identified decades ago, prior efforts to target KRAS signaling with single-agent therapeutic approaches such as farnesyl transferase inhibitors, prenylation inhibition, impairment of KRAS downstream signaling, and synthetic lethality screens have been unsuccessful. Moreover, the role of KRAS oncogene in LADC is still not fully understood, and its prognostic and predictive impact with regards to the standard of care therapy remains controversial. Of note, KRAS-related studies that included general non-small cell lung cancer (NSCLC) population instead of LADC patients should be very carefully evaluated. Recently, however, comprehensive genomic profiling and wide-spectrum analysis of other co-occurring genetic alterations have identified unique therapeutic vulnerabilities. Novel targeted agents such as the covalent KRAS G12C inhibitors or the recently proposed combinatory approaches are some examples which may allow a tailored treatment for LADC patients harboring KRAS mutations. This review summarizes the current knowledge about the therapeutic approaches of KRAS-mutated LADC and provides an update on the most recent advances in KRAS-targeted anti-cancer strategies, with a focus on potential clinical implications.
Keywords: KRAS mutation; Lung cancer; Predictive factor; Prognostic factor; Targeted therapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
