

Surgical Options for Aortic Root Replacement in Destructive Endocarditis
- PMID: 32549097
- PMCID: PMC7299601
- DOI: 10.21470/1678-9741-2020-0020
Surgical Options for Aortic Root Replacement in Destructive Endocarditis
Abstract
Objective: To analyze patients' preoperative characteristics, surgical data, postoperative courses, and short- and long-term outcomes after implantation of different full-root prostheses for destructive aortic valve endocarditis.
Methods: Between 1999 and 2018, 80 patients underwent aortic root replacement due to infective endocarditis in our institution. We analyzed the abovementioned data with standard statistical methods.
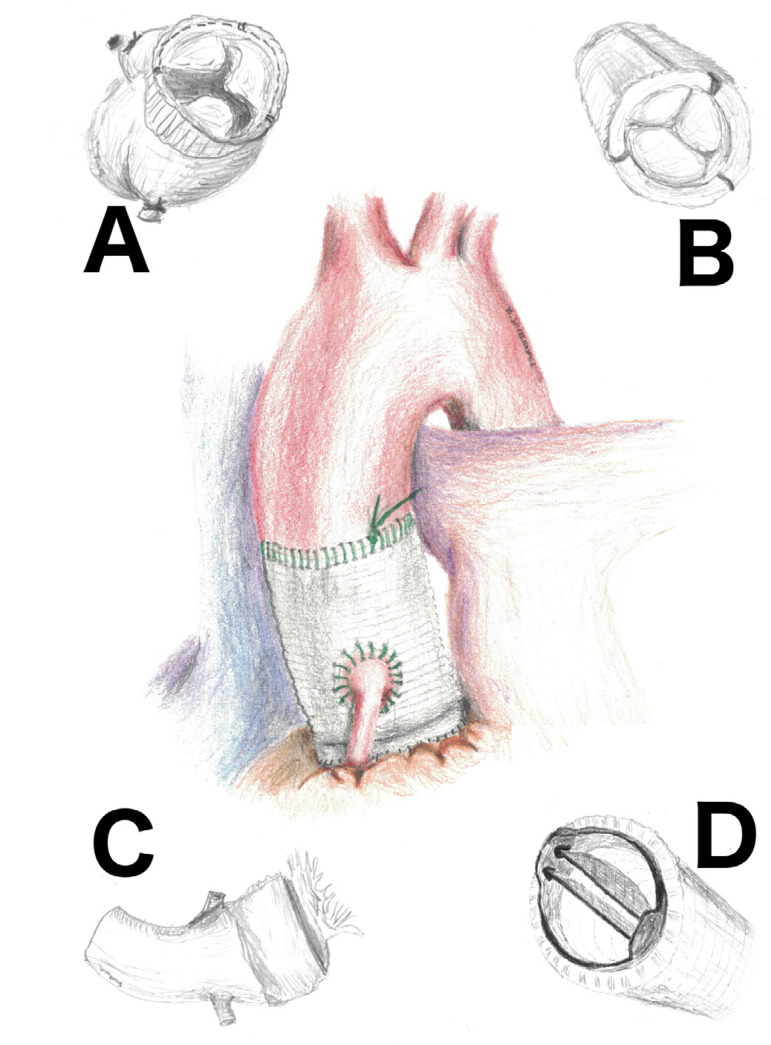
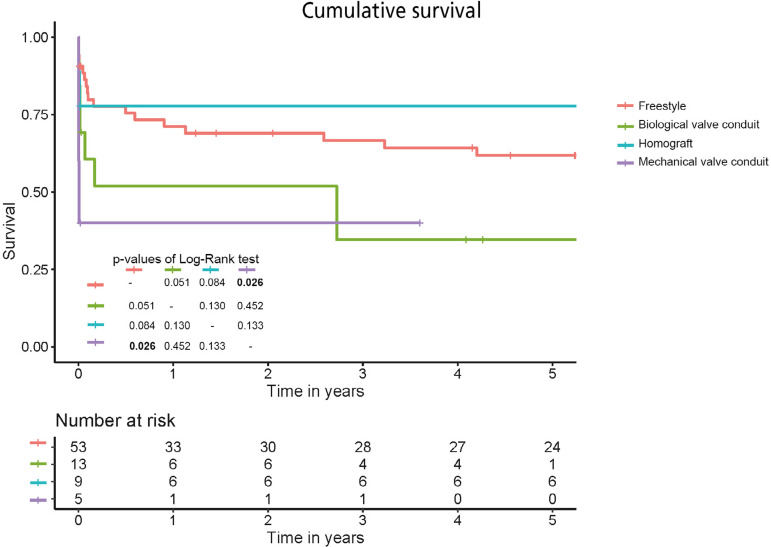
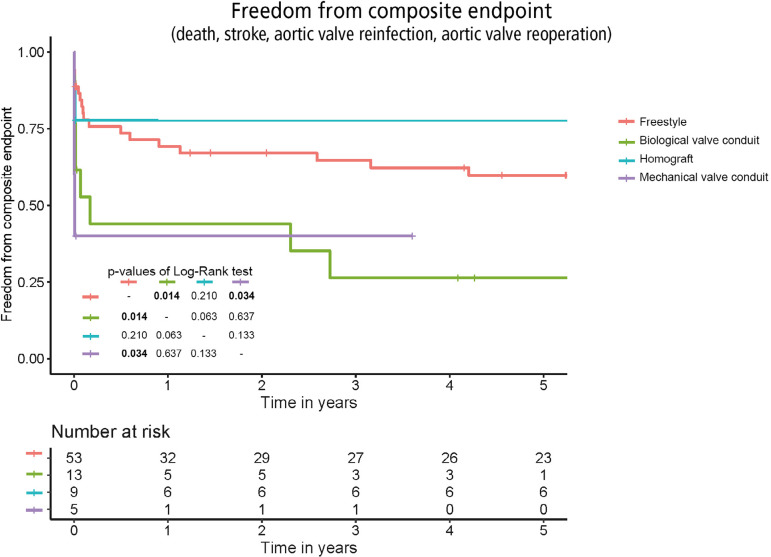
Results: The Freestyle stentless porcine prostheses were implanted in 53 (66.25%) patients, biological valve conduits in 13 (16.25%), aortic root homografts in nine (11.25%), and mechanical valve conduits in five (6.25%). There were no significant preoperative differences between the groups. The incidence of postoperative complications and intensive care unit length of stay did not differ significantly between the groups. The 30-day mortality rate was low among Freestyle patients (n=8, 15.1%) and high in the mechanical conduit cohort (n=3, 60%), though with borderline statistical significance (P=0.055). The best mean survival rates were observed after homograft (13.7 years) and stentless prosthesis (8.1 years) implantation, followed by biological (2.8 years) and mechanical (1.4 years) conduits (P=0.014). The incidence of reoperations was low in the mechanical conduit group (0) and stentless bioroot group (n=1, 1.9%), but two (15.4%) patients with biological conduits and three (33.3%) patients with homografts required reoperations in the investigated follow-up period (P=0.005).
Conclusion: In patients with the destructive form of aortic valve endocarditis, homografts and stentless porcine xenografts offer better survival rates than stented valve conduits; however, the reoperation rate among patients who received homograft valves is high.
Keywords: Allografts; Aortic Valve; Endocarditis, Bacterial; Heterografts; Reoperation; Stents; Transplantation, Heterologous.
Conflict of interest statement
No conflict of interest.
Figures
Similar articles
-
Stentless bioprostheses: a versatile and durable solution in extensive aortic valve endocarditis.Eur J Cardiothorac Surg. 2016 Jun;49(6):1699-704. doi: 10.1093/ejcts/ezv463. Epub 2016 Jan 19. Eur J Cardiothorac Surg. 2016. PMID: 26792920
-
Stentless aortic valve reoperations: a surgical challenge.Ann Thorac Surg. 2007 Sep;84(3):737-43; discussion 743-4. doi: 10.1016/j.athoracsur.2007.04.061. Ann Thorac Surg. 2007. PMID: 17720369
-
The Ross Procedure in Adults: Long-Term Results of Homografts and Stentless Xenografts for Pulmonary Valve Replacement.Thorac Cardiovasc Surg. 2017 Dec;65(8):656-661. doi: 10.1055/s-0036-1586157. Epub 2016 Aug 10. Thorac Cardiovasc Surg. 2017. PMID: 27508999
-
Homograft Versus Conventional Prosthesis for Surgical Management of Aortic Valve Infective Endocarditis: A Systematic Review and Meta-analysis.Innovations (Phila). 2018 May/Jun;13(3):163-170. doi: 10.1097/IMI.0000000000000510. Innovations (Phila). 2018. PMID: 29912740
-
In patients with severe active aortic valve endocarditis, is a stentless valve as good as the homograft?Interact Cardiovasc Thorac Surg. 2010 Sep;11(3):309-13. doi: 10.1510/icvts.2010.234831. Epub 2010 Jun 4. Interact Cardiovasc Thorac Surg. 2010. PMID: 20525759 Review.
Cited by
-
Surgical treatment of infective endocarditis in intravenous drug abusers.J Cardiothorac Surg. 2021 Apr 20;16(1):97. doi: 10.1186/s13019-021-01491-1. J Cardiothorac Surg. 2021. PMID: 33879196 Free PMC article.
-
Contemporary surgical management of infective endocarditis of the aortic root.Indian J Thorac Cardiovasc Surg. 2024 May;40(Suppl 1):83-92. doi: 10.1007/s12055-023-01604-6. Epub 2023 Oct 19. Indian J Thorac Cardiovasc Surg. 2024. PMID: 38827543 Free PMC article. Review.
-
The Surgical Treatment of Infective Endocarditis: A Comprehensive Review.Diagnostics (Basel). 2024 Feb 20;14(5):464. doi: 10.3390/diagnostics14050464. Diagnostics (Basel). 2024. PMID: 38472937 Free PMC article. Review.
-
Choice of valve substitutes.Indian J Thorac Cardiovasc Surg. 2024 May;40(Suppl 1):78-82. doi: 10.1007/s12055-024-01733-6. Epub 2024 Apr 29. Indian J Thorac Cardiovasc Surg. 2024. PMID: 38827545 Free PMC article. Review.
References
-
- Anantha Narayanan M, Mahfood Haddad T, Kalil AC, Kanmanthareddy A, Suri RM, Mansour G, et al. Early versus late surgical intervention or medical management for infective endocarditis: a systematic review and metaanalysis. Heart. 2016;102(12):950–957. doi: 10.1136/heartjnl-2015-308589. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical