

A Surgical Technique to Repair Perineal Body Disruption Secondary to Sexual Assault
- PMID: 32550122
- PMCID: PMC7188516
- DOI: 10.1055/s-0039-1695048
A Surgical Technique to Repair Perineal Body Disruption Secondary to Sexual Assault
Abstract
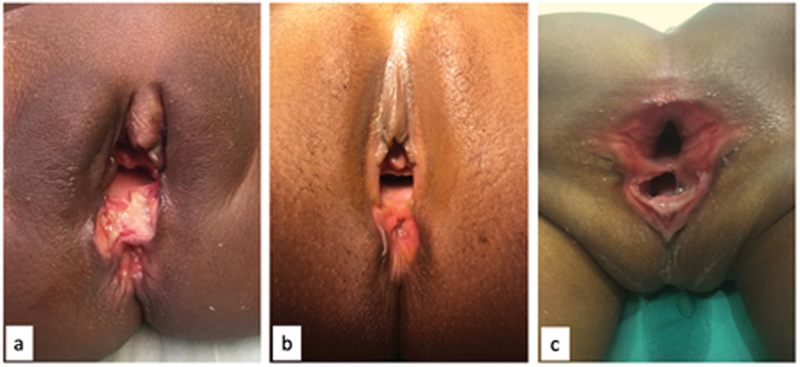
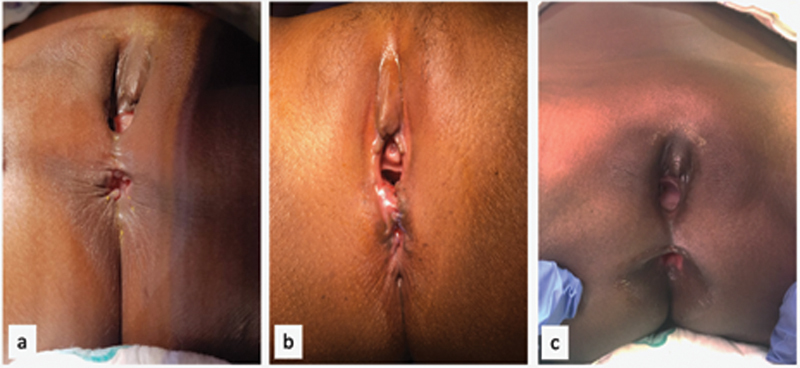
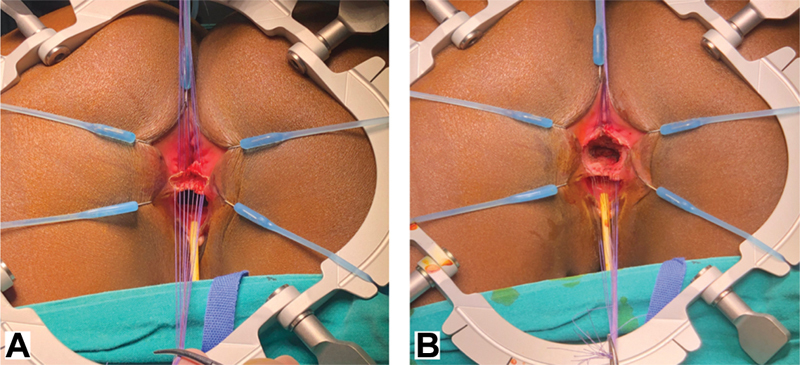
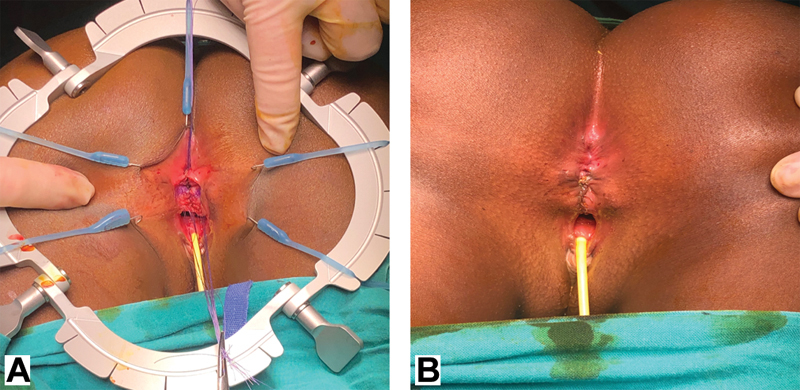
Perineal trauma is uncommon in the pediatric population and it is estimated that 5 to 21% is secondary to sexual abuse. We aim to present a proposed surgical technique to repair perineal injuries secondary to sexual assault in female children. The technique is based on the posterior sagittal anorectoplasty (PSARP) for repairing anorectal malformations and, between 2017 and 2019, it was used to treat three girls (2 months, 2 years, and 8 years of age) with fourth-degree perineal injuries secondary to sexual assault. One of them underwent laparotomy and Hartmann's colostomy for an acute abdomen. Two underwent wound debridement and suturing and only had a stoma fashioned at 5 days and 6 weeks posttrauma, respectively. The perineal repair was performed 2, 6, and 7 weeks postinjury and done as follows: with the child prone in jack-knife position, stay-sutures are placed on the common wall between the rectum and the vagina. Using a needle tip diathermy, a transverse incision is performed below the sutures lifting the anterior rectal wall up. Stay sutures are then positioned on the posterior wall of the vaginal mucosa. The incision between the walls is deepened until the rectum and the vagina are completely separated. The deep and superficial perineal body is then reconstructed using absorbable sutures and an anterior anoplasty and an introitoplasty are performed. The stoma in each was closed 6 weeks postreconstruction. At follow-up, now 1 year or more postrepair, all patients have an excellent cosmetic outcome and are fully continent for stools.
Keywords: perineal injury; perineal reconstruction; perineal trauma; posterior sagittal anorectoplasty; sexual assault.
Conflict of interest statement
Conflict of Interest None declared.
Figures


References
-
- Onen A, Oztürk H, Yayla M, Basuguy E, Gedik S. Genital trauma in children: classification and management. Urology. 2005;65(05):986–990. - PubMed
-
- Janssen T L, van Dijk M, Al Malki I, van As A B. Management of physical child abuse in South Africa: literature review and children's hospital data analysis. Paediatr Int Child Health. 2013;33(04):216–227. - PubMed
-
- Scheidler M G, Schultz B L, Schall L, Ford H R. Mechanisms of blunt perineal injury in female pediatric patients. J Pediatr Surg. 2000;35(09):1317–1319. - PubMed
-
- Russell K W, Soukup E S, Metzger R R et al. Fecal continence following complex anorectal trauma in children. J Pediatr Surg. 2014;49(02):349–352. - PubMed
-
- Bakal U, Sarac M, Tartar T, Cigsar E B, Kazez A. Twenty years of experience with perineal injury in children. Eur J Trauma Emerg Surg. 2016;42(05):599–603. - PubMed
Publication types
LinkOut - more resources
Full Text Sources