

Adjusted tight control blood glucose management in diabetic patients undergoing on pump coronary artery bypass graft. A randomized clinical trial
- PMID: 32550193
- PMCID: PMC7270305
- DOI: 10.1007/s40200-020-00494-4
Adjusted tight control blood glucose management in diabetic patients undergoing on pump coronary artery bypass graft. A randomized clinical trial
Erratum in
-
Correction to: Adjusted tight control blood glucose management in diabetic patients undergoing on pump coronary artery bypass graft. A randomized clinical trial.J Diabetes Metab Disord. 2020 Feb 7;19(1):665. doi: 10.1007/s40200-020-00500-9. eCollection 2020 Jun. J Diabetes Metab Disord. 2020. PMID: 32550640 Free PMC article.
Abstract
Background: Many of the patients who are undergoing Coronary Artery Bypass Graft have diabetes mellitus or metabolic syndrome and are at risk for hyperglycemia events.
Objective: The present study aimed to compare conventional glucose control with adjusted tight control in patients undergoing on-pump CABG.
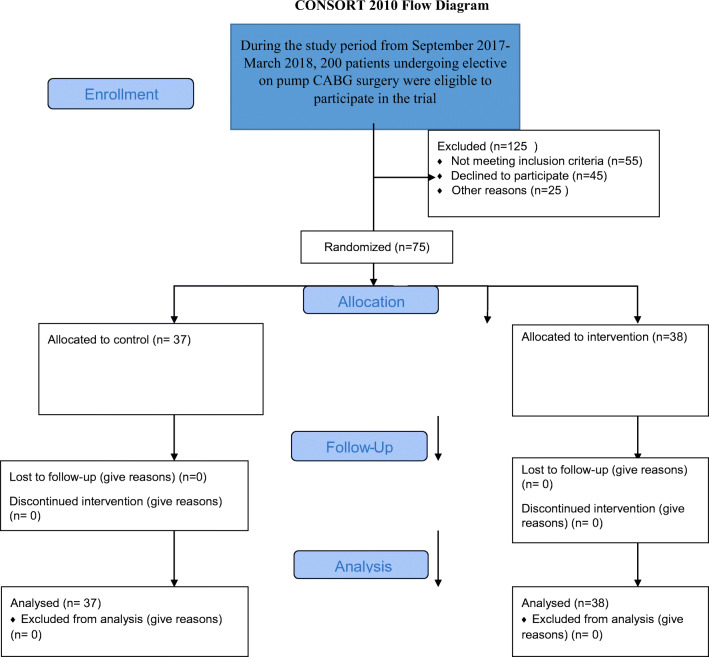
Methods: This double -blind randomized clinical trial study was conducted in Shiraz, Iran, from September 2017-March 2018. Two consecutive groups of 75 patients undergoing elective on- pump coronary artery bypass graft surgery.
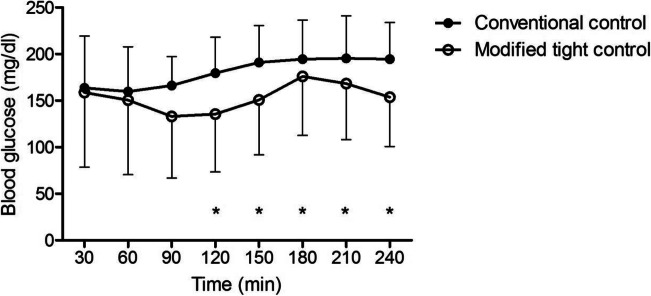
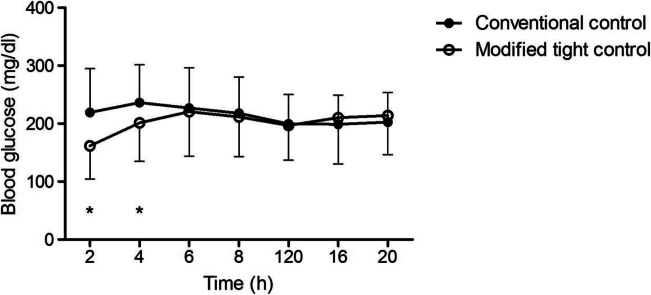
Intervention: The patients were divided into adjusted tight control of the blood glucose between 100 and 120 mg/dl and conventional method that the blood glucose maintained ≤200 mg/dl.
Primary outcomes were: mortality, sternal wound infection, cardiac arrhythmia, cerebrovascular attack, and acute renal failure.
Secondary outcomes included: duration of mechanical ventilation and length of ICU staying. The same main outcomes were evaluated after one month.
Statistical analysis: The data were analyzed using SPSS version 20(SPSS, Chicago, IL). Group comparisons were performed using t-tests and Chi-square tests. Repeated measurement test was used for comparing blood glucose in two groups. Mann Whitney U test was compared duration of the mechanical ventilation and length of ICU staying. Statistical significance was defined as a p value <0.05.
Results: There were no significant differences between main and secondary outcomes. About late outcomes, sternal wound infection was in the control group (7 patients) more than intervention (1 patient) (P < 0.05). No differences between other complications in both groups were observed. The occurrence of hypoglycemia was low in both groups. Hypokalemia was significantly higher in the intervention than in control (P < 0.001).
Conclusions: The findings showed using adjusted tight glycemic control to a level that is nearby to normal values during cardiac surgery may reduce episodes of hypoglycemia and thus reduces its side effects. As well as reduce hyperglycemic complications such as sternal wound infection.
Trial registration number: IRCT2013041713052N1). 2013-07-09.
Keywords: Cardiac surgery; Critically ill patient; Diabetes; Tight control of glucose.
© Springer Nature Switzerland AG 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.Conflicting interestThere is no conflict of interest to be declared.
Figures
References
-
- Gorter PM, Olijhoek JK, van der Graaf Y, Algra A, Rabelink TJ, Visseren FL, et al. Prevalence of the metabolic syndrome in patients with coronary heart disease, cerebrovascular disease, peripheral arterial disease or abdominal aortic aneurysm. Atherosclerosis. 2004;173(2):361–367. doi: 10.1016/j.atherosclerosis.2003.12.033. - DOI - PubMed
-
- Doenst T, Wijeysundera D, Karkouti K, Zechner C, Maganti M, Rao V, et al. Hyperglycemia during cardiopulmonary bypass is an independent risk factor for mortality in patients undergoing cardiac surgery. The Journal of thoracic and cardiovascular surgery. 2005;130(4):e1–e8. doi: 10.1016/j.jtcvs.2005.05.049. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
