

Pathological Findings of Postmortem Biopsies From Lung, Heart, and Liver of 7 Deceased COVID-19 Patients
- PMID: 32552178
- PMCID: PMC8041443
- DOI: 10.1177/1066896920935195
Pathological Findings of Postmortem Biopsies From Lung, Heart, and Liver of 7 Deceased COVID-19 Patients
Abstract
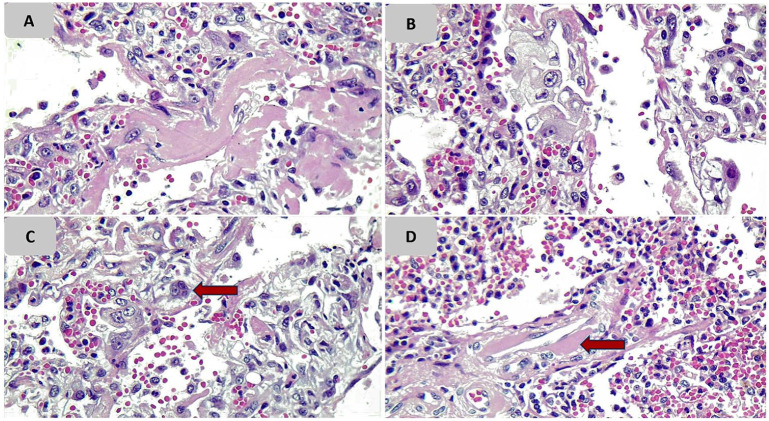
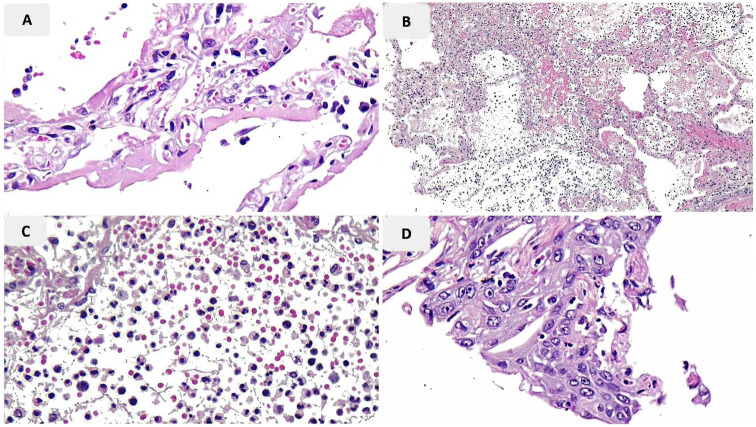
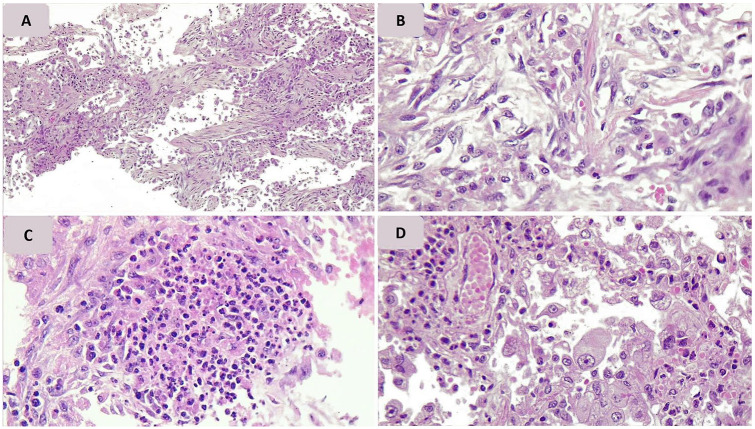
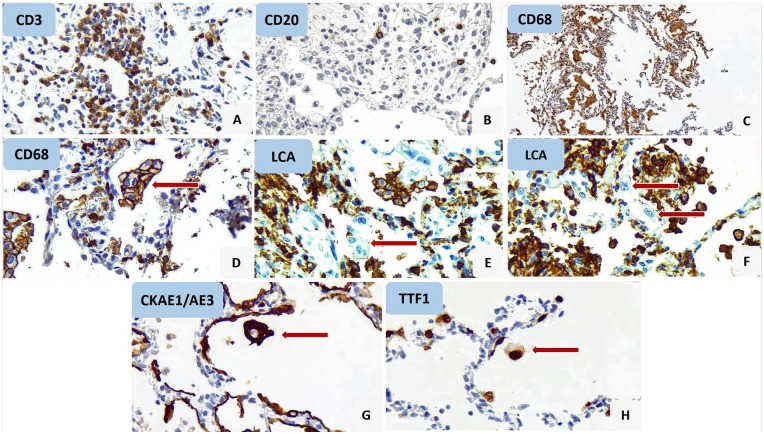
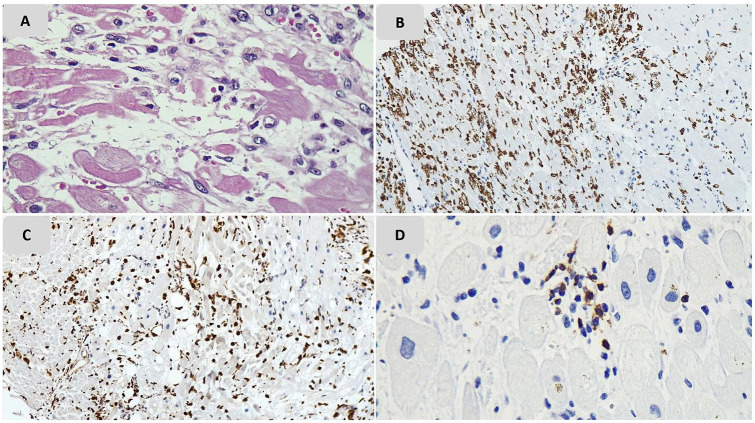
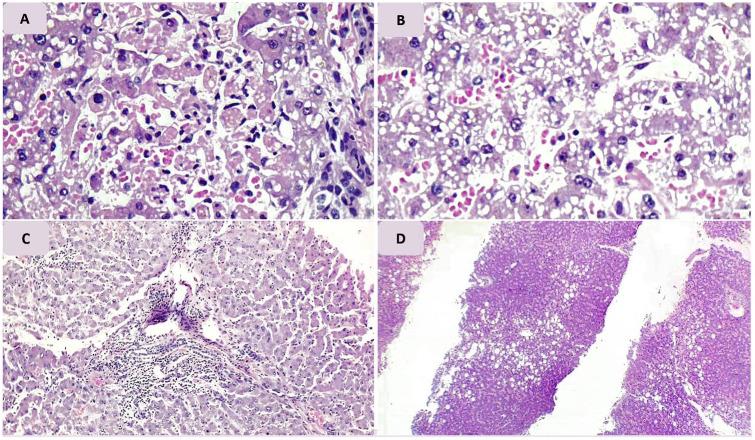
Background. A novel coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been affecting almost all nations around the world. Most infected patients who have been admitted to intensive care units show SARS signs. In this study, we aimed to achieve a better understanding of pathological alterations that take place during the novel coronavirus infection in most presumed affected organs. Methods. We performed postmortem core needle biopsies from lung, heart, and liver on 7 deceased patients who had died of coronavirus disease 2019. Prepared tissue sections were observed by 2 expert pathologists. Results. Diffuse alveolar damage was the main pathologic finding in the lung tissue samples. Patients with hospitalization durations of more than 10 days showed evidence of organization. Multinucleated cells in alveolar spaces and alveolar walls, atypical enlarged cells, accumulation of macrophages in alveolar spaces, and congestion of vascular channels were the other histopathologic alteration of the lung. None of our heart biopsy samples met the criteria for myocarditis. Liver biopsies showed congestion, micro- and macro-vesicular changes, and minimal to mild portal inflammation, in the majority of cases. Conclusions. Similar to the previous coronavirus infection in 2003, the main pathologic finding in the lung was diffuse alveolar damage with a pattern of organization in prolonged cases. The SARS-CoV-2 infection does not cause myocarditis, and the ischemia of myocardium is the most probable justification of the observed pathologic changes in the heart. Liver tissue sections mostly showed nonspecific findings; however, ischemia of the liver can be identified in some cases.
Keywords: COVID-19; lung; pathology; postmortem examination; severe acute respiratory syndrome coronavirus 2.
Conflict of interest statement
Figures
Similar articles
-
Diffuse alveolar damage and thrombotic microangiopathy are the main histopathological findings in lung tissue biopsy samples of COVID-19 patients.Pathol Res Pract. 2020 Oct;216(10):153228. doi: 10.1016/j.prp.2020.153228. Epub 2020 Sep 19. Pathol Res Pract. 2020. PMID: 32979740 Free PMC article.
-
Postmortem lung biopsies from four patients with COVID-19 at a tertiary hospital in Cape Town, South Africa.S Afr Med J. 2020 Oct 19;110(12):1195-1200. doi: 10.7196/SAMJ.2020.v110i12.15290. S Afr Med J. 2020. PMID: 33403965
-
[A pathological report of three COVID-19 cases by minimal invasive autopsies].Zhonghua Bing Li Xue Za Zhi. 2020 May 8;49(5):411-417. doi: 10.3760/cma.j.cn112151-20200312-00193. Zhonghua Bing Li Xue Za Zhi. 2020. PMID: 32172546 Chinese.
-
A review of the main histopathological findings in coronavirus disease 2019.Hum Pathol. 2020 Nov;105:74-83. doi: 10.1016/j.humpath.2020.07.023. Epub 2020 Aug 2. Hum Pathol. 2020. PMID: 32750378 Free PMC article.
-
Pathological Evidence for SARS-CoV-2 as a Cause of Myocarditis: JACC Review Topic of the Week.J Am Coll Cardiol. 2021 Jan 26;77(3):314-325. doi: 10.1016/j.jacc.2020.11.031. J Am Coll Cardiol. 2021. PMID: 33478655 Free PMC article. Review.
Cited by
-
Implications of microscale lung damage for COVID-19 pulmonary ventilation dynamics: A narrative review.Life Sci. 2021 Jun 1;274:119341. doi: 10.1016/j.lfs.2021.119341. Epub 2021 Mar 11. Life Sci. 2021. PMID: 33716059 Free PMC article. Review.
-
Histopathological Findings in COVID-19 Cases: A Systematic Review.Cureus. 2022 Jun 1;14(6):e25573. doi: 10.7759/cureus.25573. eCollection 2022 Jun. Cureus. 2022. PMID: 35784976 Free PMC article. Review.
-
Minimally Invasive Tissue Sampling Findings in 12 Patients With Coronavirus Disease 2019.Clin Infect Dis. 2021 Dec 15;73(Suppl_5):S454-S464. doi: 10.1093/cid/ciab812. Clin Infect Dis. 2021. PMID: 34910166 Free PMC article.
-
Serum Amyloid P inhibits single stranded RNA-induced lung inflammation, lung damage, and cytokine storm in mice.PLoS One. 2021 Jan 22;16(1):e0245924. doi: 10.1371/journal.pone.0245924. eCollection 2021. PLoS One. 2021. PMID: 33481950 Free PMC article.
-
Cellular and molecular features of COVID-19 associated ARDS: therapeutic relevance.J Inflamm (Lond). 2023 Mar 20;20(1):11. doi: 10.1186/s12950-023-00333-2. J Inflamm (Lond). 2023. PMID: 36941580 Free PMC article. Review.
References
-
- Wuhan Municipal Health Commission. Report of Clustering Pneumonia of Unknown Etiology in Wuhan City. Municipal Health Commission; 2019.
-
- World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it. Accessed June 2, 2019. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technica...
-
- World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19—11 March 2020. Accessed June 5, 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
