

Successful Outcomes of Newly Diagnosed T Lymphoblastic Lymphoma: Results From Children's Oncology Group AALL0434
- PMID: 32552472
- PMCID: PMC7479761
- DOI: 10.1200/JCO.20.00531
Successful Outcomes of Newly Diagnosed T Lymphoblastic Lymphoma: Results From Children's Oncology Group AALL0434
Erratum in
-
Erratum: Successful Outcomes of Newly Diagnosed T Lymphoblastic Lymphoma: Results From Children's Oncology Group AALL0434.J Clin Oncol. 2026 Jan 5:JCO2502779. doi: 10.1200/JCO-25-02779. Online ahead of print. J Clin Oncol. 2026. PMID: 41490480 No abstract available.
Abstract
Purpose: The Children's Oncology Group (COG) protocol AALL0434 evaluated the safety and efficacy of multi-agent chemotherapy with Capizzi-based methotrexate/pegaspargase (C-MTX) in patients with newly diagnosed pediatric T-cell lymphoblastic lymphoma (T-LL) and gained preliminary data using nelarabine in high-risk patients.
Patients and methods: The trial enrolled 299 patients, age 1-31 years. High-risk (HR) patients had ≥ 1% minimal detectable disease (MDD) in the bone marrow at diagnosis or received prior steroid treatment. Induction failure was defined as failure to achieve a partial response (PR) by the end of the 4-week induction. All patients received the augmented Berlin-Frankfurt-Muenster (ABFM) C-MTX regimen. HR patients were randomly assigned to receive or not receive 6 5-day courses of nelarabine incorporated into ABFM. Patients with induction failure were nonrandomly assigned to ABFM C-MTX plus nelarabine. No patients received prophylactic cranial radiation; however, patients with CNS3 disease (CSF WBC ≥ 5/μL with blasts or cranial nerve palsies, brain/eye involvement, or hypothalamic syndrome) were ineligible.
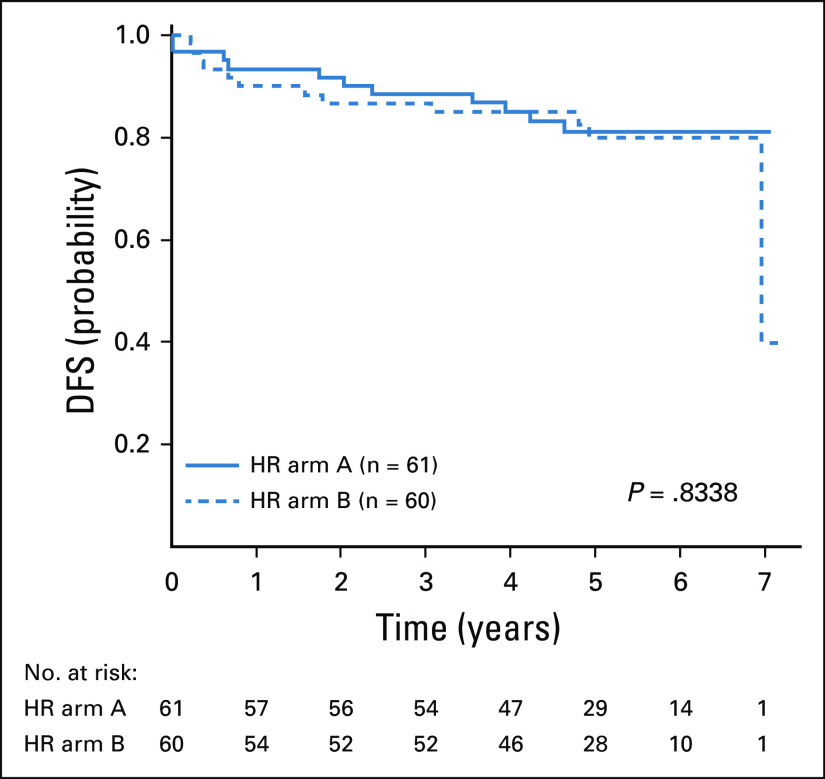
Results: At end-induction, 98.8% of evaluable participants had at least a PR. The 4-year event-free survival (EFS) and overall survival (OS) were 84.7% ± 2.3% and 89.0% ± 2.0%. The 4-year disease-free survival (DFS) from end-induction was 85.9% ± 2.6%. There was no difference in DFS observed between the HR and standard-risk groups (P = .29) or by treatment regimen (P = .55). Disease stage, tumor response, and MDD at diagnosis did not demonstrate thresholds that resulted in differences in EFS. Nelarabine did not show an advantage for HR patients. CNS relapse occurred in only 4 patients.
Conclusion: COG AALL0434 produced excellent outcomes in one of the largest trials ever conducted for patients with newly diagnosed T-LL. The COG ABFM regimen with C-MTX provided excellent EFS and OS without cranial radiation.
Trial registration: ClinicalTrials.gov NCT00408005.
Figures






References
-
- Heerema NA, Sather HN, Sensel MG, et al. Frequency and clinical significance of cytogenetic abnormalities in pediatric T-lineage acute lymphoblastic leukemia: A report from the Children’s Cancer Group. J Clin Oncol. 1998;16:1270–1278. - PubMed
-
- Lones MA, Heerema NA, Le Beau MM, et al. Chromosome abnormalities in advanced stage lymphoblastic lymphoma of children and adolescents: A report from CCG-E08. Cancer Genet Cytogenet. 2007;172:1–11. - PubMed
-
- Balbach ST, Makarova O, Bonn BR, et al. Proposal of a genetic classifier for risk group stratification in pediatric T-cell lymphoblastic lymphoma reveals differences from adult T-cell lymphoblastic leukemia. Leukemia. 2016;30:970–973. - PubMed
-
- Callens C, Baleydier F, Lengline E, et al. Clinical impact of NOTCH1 and/or FBXW7 mutations, FLASH deletion, and TCR status in pediatric T-cell lymphoblastic lymphoma. J Clin Oncol. 2012;30:1966–1973. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
