

The ReWalk ReStore™ soft robotic exosuit: a multi-site clinical trial of the safety, reliability, and feasibility of exosuit-augmented post-stroke gait rehabilitation
- PMID: 32552775
- PMCID: PMC7301475
- DOI: 10.1186/s12984-020-00702-5
The ReWalk ReStore™ soft robotic exosuit: a multi-site clinical trial of the safety, reliability, and feasibility of exosuit-augmented post-stroke gait rehabilitation
Abstract
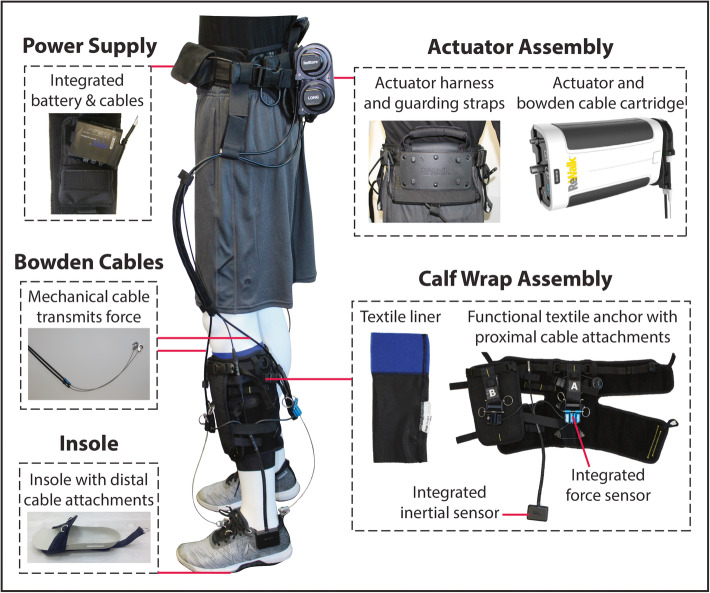
Background: Atypical walking in the months and years after stroke constrain community reintegration and reduce mobility, health, and quality of life. The ReWalk ReStore™ is a soft robotic exosuit designed to assist the propulsion and ground clearance subtasks of post-stroke walking by actively assisting paretic ankle plantarflexion and dorsiflexion. Previous proof-of-concept evaluations of the technology demonstrated improved gait mechanics and energetics and faster and farther walking in users with post-stroke hemiparesis. We sought to determine the safety, reliability, and feasibility of using the ReStore™ during post-stroke rehabilitation.
Methods: A multi-site clinical trial (NCT03499210) was conducted in preparation for an application to the United States Food and Drug Administration (FDA). The study included 44 users with post-stroke hemiparesis who completed up to 5 days of training with the ReStore™ on the treadmill and over ground. In addition to primary and secondary endpoints of safety and device reliability across all training activities, an exploratory evaluation of the effect of multiple exposures to using the device on users' maximum walking speeds with and without the device was conducted prior to and following the five training visits.
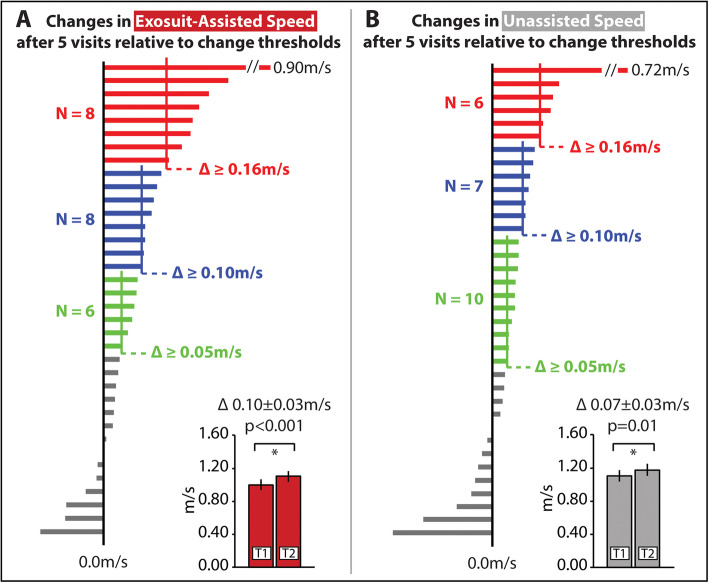
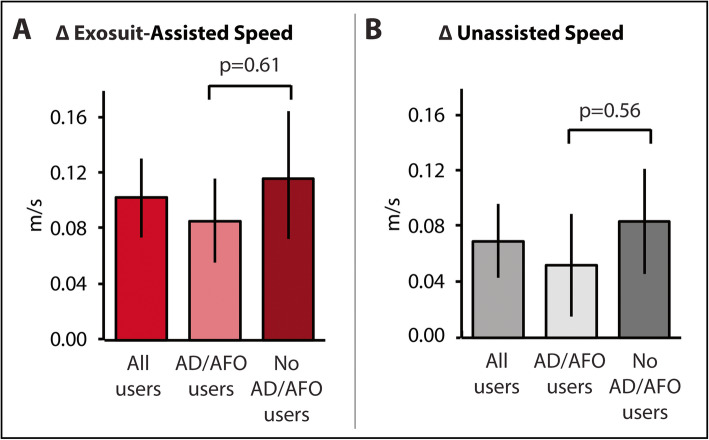
Results: All 44 study participants completed safety and reliability evaluations. Thirty-six study participants completed all five training days. No device-related falls or serious adverse events were reported. A low rate of device malfunctions was reported by clinician-operators. Regardless of their reliance on ancillary assistive devices, after only 5 days of walking practice with the device, study participants increased both their device-assisted (Δ: 0.10 ± 0.03 m/s) and unassisted (Δ: 0.07 ± 0.03 m/s) maximum walking speeds (P's < 0.05).
Conclusions: When used under the direction of a licensed physical therapist, the ReStore™ soft exosuit is safe and reliable for use during post-stroke gait rehabilitation to provide targeted assistance of both paretic ankle plantarflexion and dorsiflexion during treadmill and overground walking.
Trial registration: NCT03499210. Prospectively registered on March 28, 2018.
Keywords: Exoskeleton; Exosuit; Physical therapy; Rehabilitation; Stroke; Walking.
Conflict of interest statement
The authors were the site principal investigators for the multi-site clinical trial. The authors declare that the trial was funded by the device manufacturer; however, none of the authors have personal financial interests or conflicts with the subject matter.
Figures
References
-
- Winter DA. Biomechanics and motor control of human gait: normal, elderly and pathological. Waterloo: University of Waterloo Press; 1991.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
