

Methods to identify dementia in the electronic health record: Comparing cognitive test scores with dementia algorithms
- PMID: 32553526
- PMCID: PMC7363308
- DOI: 10.1016/j.hjdsi.2020.100430
Methods to identify dementia in the electronic health record: Comparing cognitive test scores with dementia algorithms
Abstract
Background: Epidemiologic studies often use diagnosis codes to identify dementia outcomes. It remains unknown to what extent cognitive screening test results add value in identifying dementia cases in big data studies leveraging electronic health record (EHR) data. We examined test scores from EHR data and compared results with dementia algorithms.
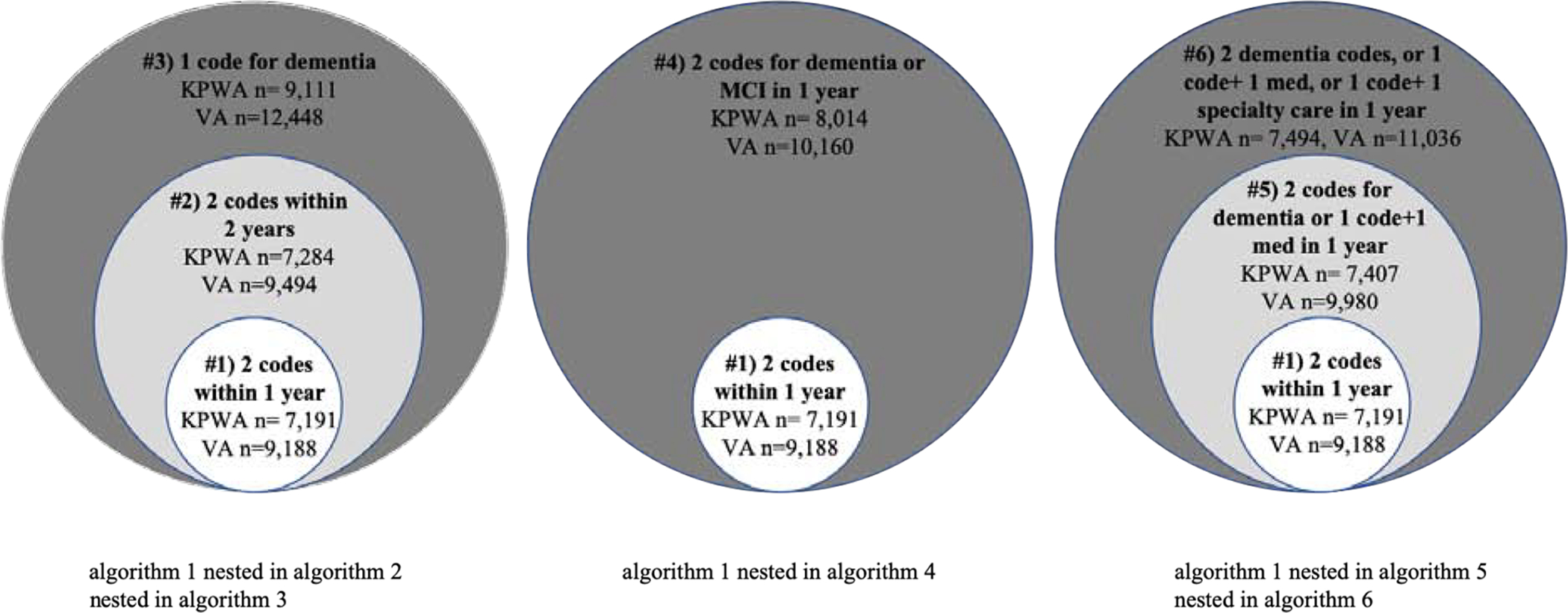
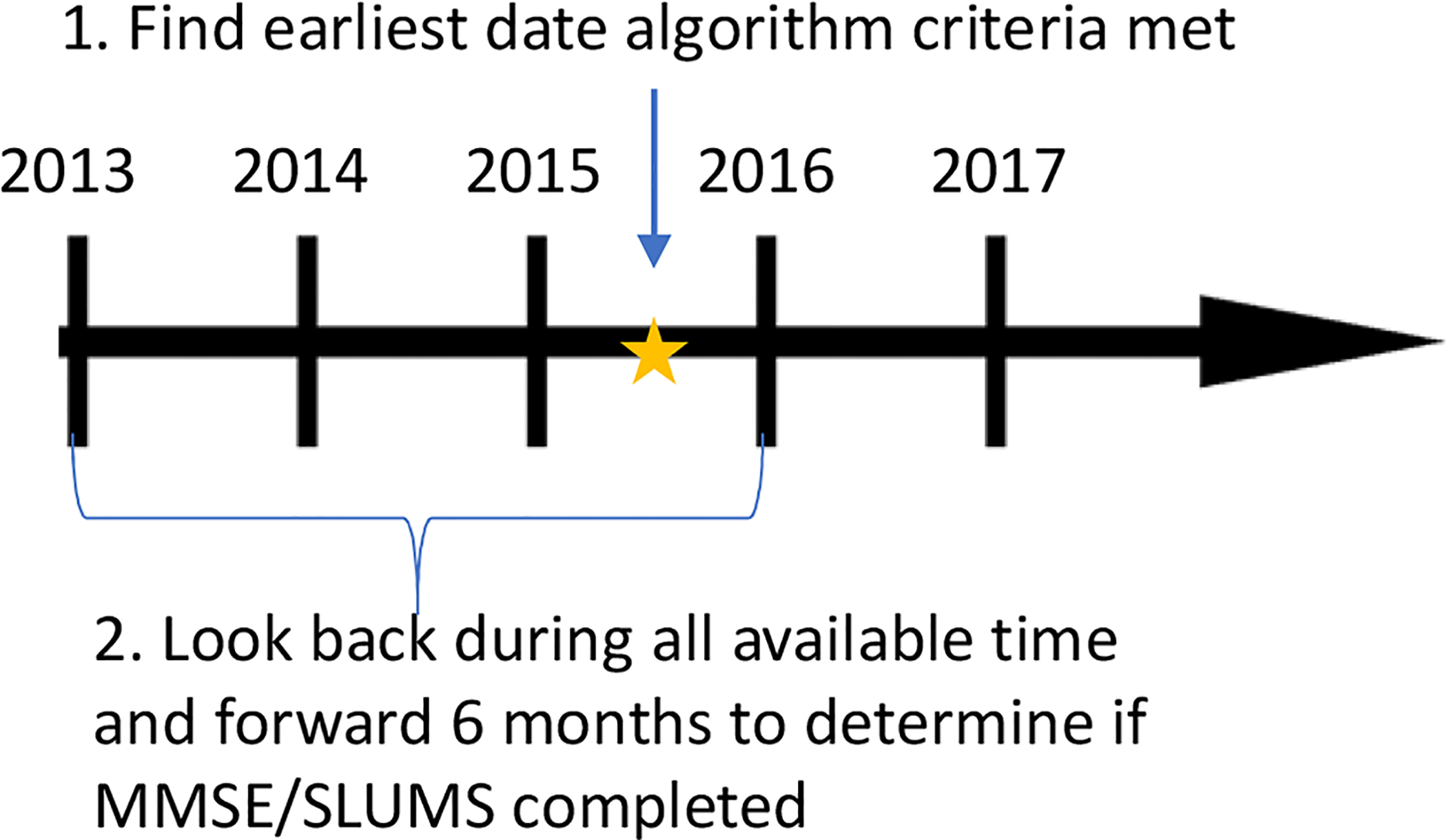
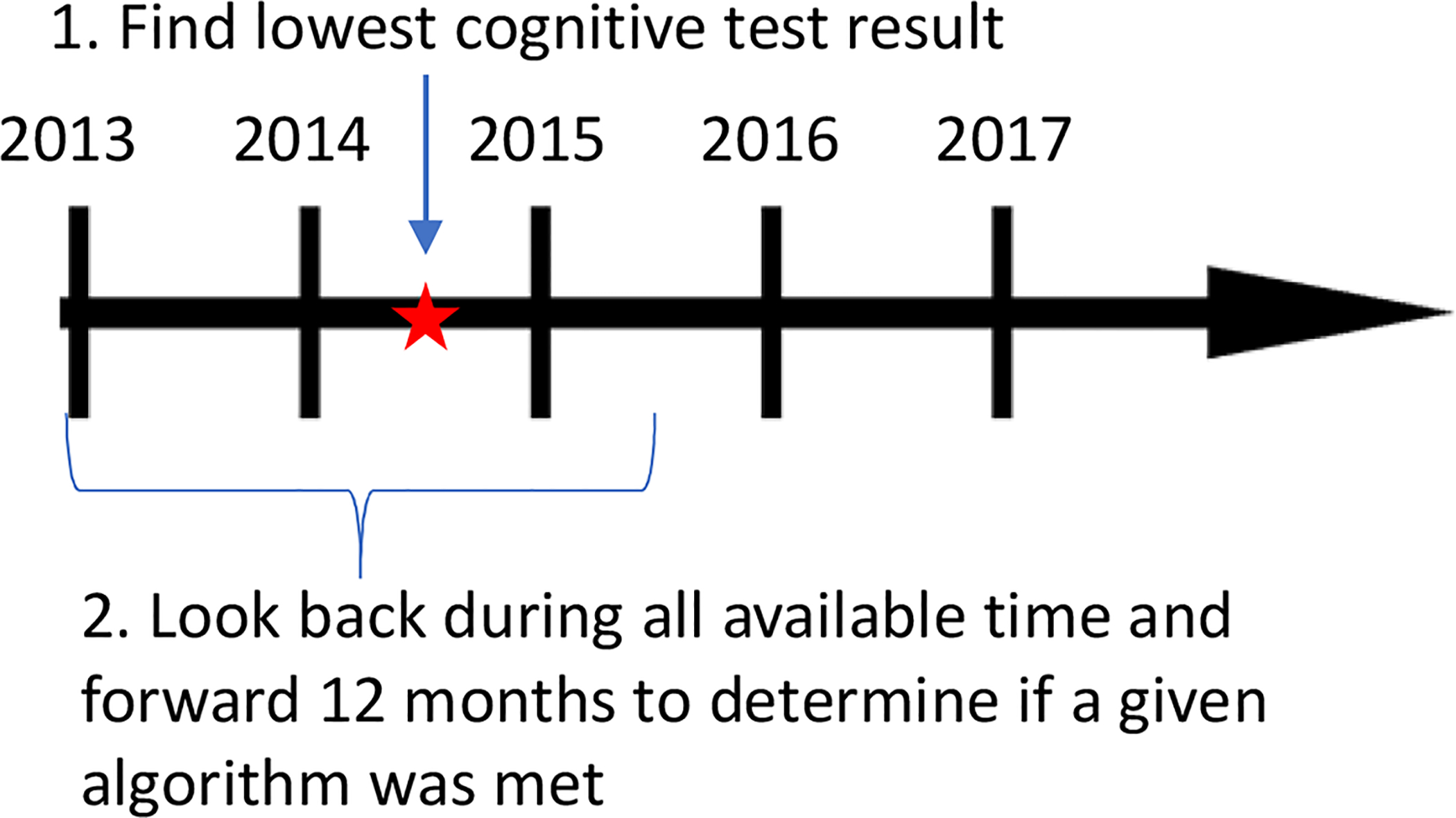
Methods: This retrospective cohort study included patients 60+ years of age from Kaiser Permanente Washington (KPWA) during 2013-2018 and the Veterans Health Affairs (VHA) during 2012-2015. Results from the Mini Mental State Examination (MMSE) and the Saint Louis University Mental Status Examination (SLUMS) cognitive screening exams, were classified as showing dementia or not. Multiple dementia algorithms were created using combinations of diagnosis codes, pharmacy records, and specialty care visits. Correlations between test scores and algorithms were assessed.
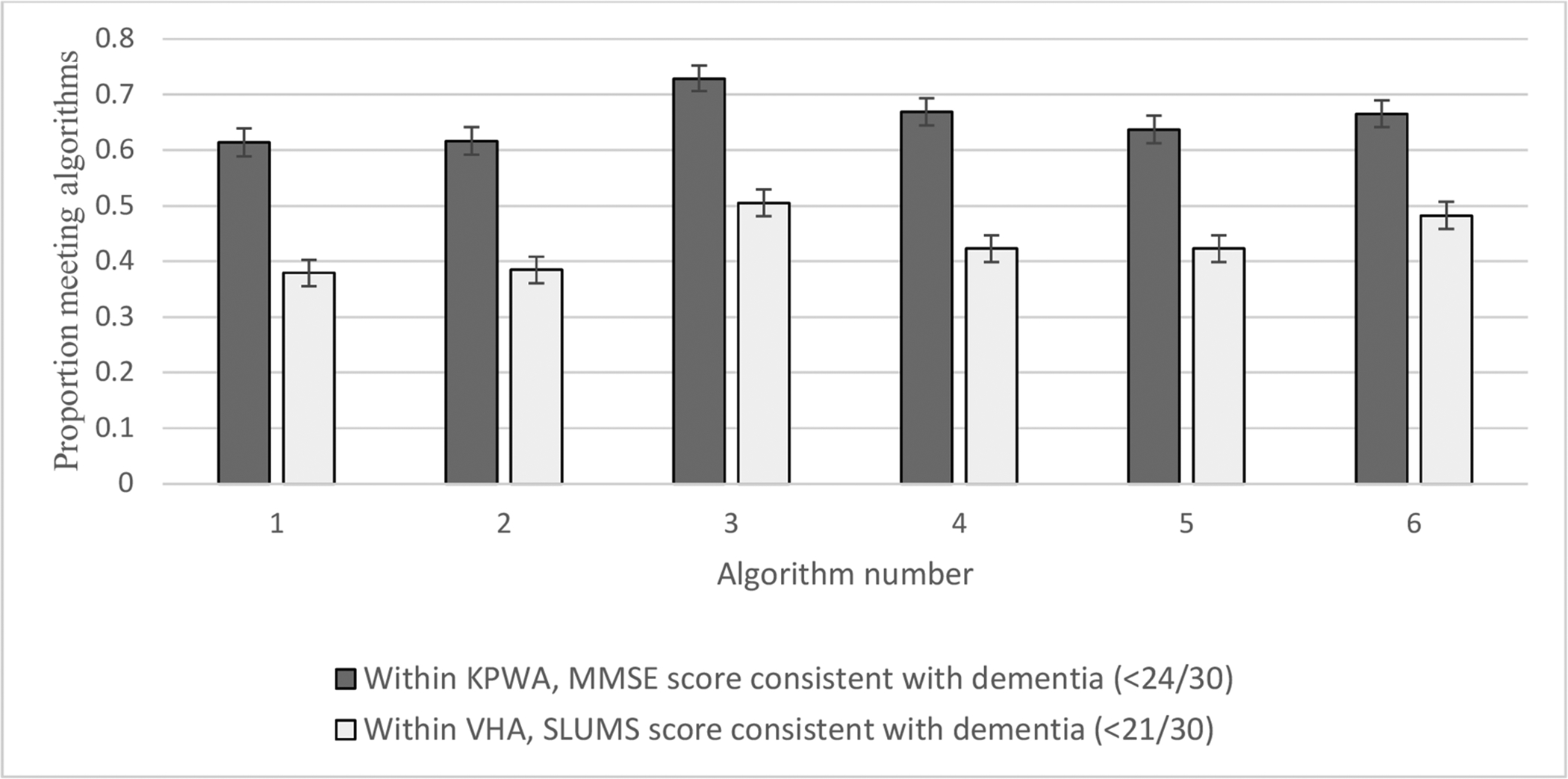
Results: 3,690 of 112,917 KPWA patients and 2,981 of 102,981 VHA patients had cognitive test results in the EHR. In KPWA, dementia prevalence ranged from 6.4%-8.1% depending on the algorithm used and in the VHA, 8.9%-12.1%. The algorithm which best agreed with test scores required ≥2 dementia diagnosis codes in 12 months; at KPWA, 14.8% of people meeting this algorithm had an MMSE score, of whom 65% had a score indicating dementia. Within VHA, those figures were 6.2% and 77% respectively.
Conclusions: Although cognitive test results were rarely available, agreement was good with algorithms requiring ≥2 dementia diagnosis codes, supporting the accuracy of this algorithm.
Implications: These scores may add value in identifying dementia cases for EHR-based research studies.
Keywords: Algorithms; Cognitive screening; Dementia; Electronic health record.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest Dr. Floyd has consulted for Shionogi Inc. Other authors have no conflicts of interest to disclose.
Figures
References
-
- Chodosh J, et al. , Physician recognition of cognitive impairment: evaluating the need for improvement. J Am Geriatr Soc, 2004. 52(7): p. 1051–9. - PubMed
-
- Querfurth HW and LaFerla FM, Alzheimer’s disease. N Engl J Med, 2010. 362(4): p. 329–44. - PubMed
-
- Reuben DB, et al. , An Automated Approach to Identifying Patients with Dementia Using Electronic Medical Records. J Am Geriatr Soc, 2017. 65(3): p. 658–659. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
