

COVID-19 and the liver
- PMID: 32553666
- PMCID: PMC7295524
- DOI: 10.1016/j.jhep.2020.06.006
COVID-19 and the liver
Abstract
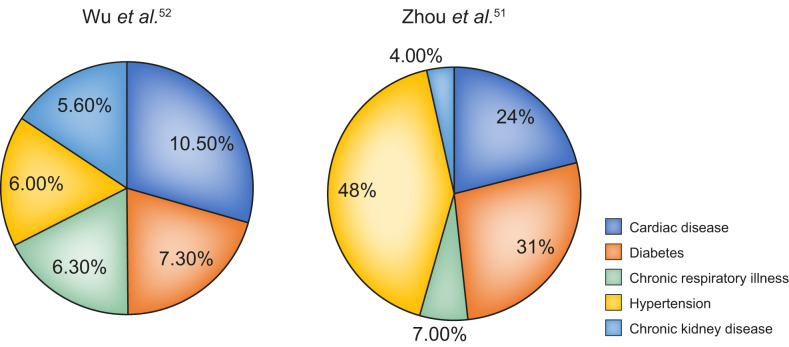
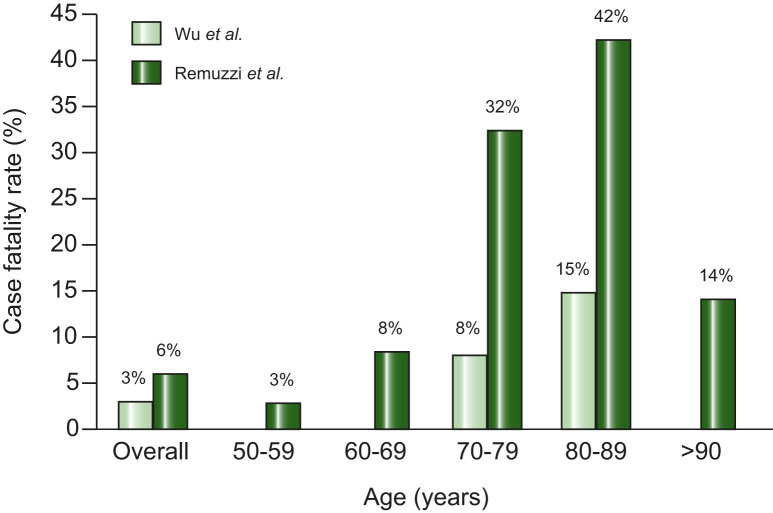
The current coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), has become a major public health crisis over the past few months. Overall case fatality rates range between 2-6%; however, the rates are higher in the elderly and those with underlying comorbidities like diabetes, hypertension and heart disease. Recent reports showed that about 2-11% of patients with COVID-19 had underlying chronic liver disease. During the previous SARS epidemic, around 60% of patients were reported to develop various degrees of liver damage. In the current pandemic, hepatic dysfunction has been seen in 14-53% of patients with COVID-19, particularly in those with severe disease. Cases of acute liver injury have been reported and are associated with higher mortality. Hepatic involvement in COVID-19 could be related to the direct cytopathic effect of the virus, an uncontrolled immune reaction, sepsis or drug-induced liver injury. The postulated mechanism of viral entry is through the host angiotensin-converting enzyme 2 (ACE2) receptors that are abundantly present in type 2 alveolar cells. Interestingly, ACE2 receptors are expressed in the gastrointestinal tract, vascular endothelium and cholangiocytes of the liver. The effects of COVID-19 on underlying chronic liver disease require detailed evaluation and, with data currently lacking, further research is warranted in this area.
Keywords: ACE2; COVID-19; Liver; SARS-CoV-2.
Copyright © 2020 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
