

Clinical and Genomic Epidemiology of Carbapenem-Nonsusceptible Citrobacter spp. at a Tertiary Health Care Center over 2 Decades
- PMID: 32554477
- PMCID: PMC7448640
- DOI: 10.1128/JCM.00275-20
Clinical and Genomic Epidemiology of Carbapenem-Nonsusceptible Citrobacter spp. at a Tertiary Health Care Center over 2 Decades
Abstract
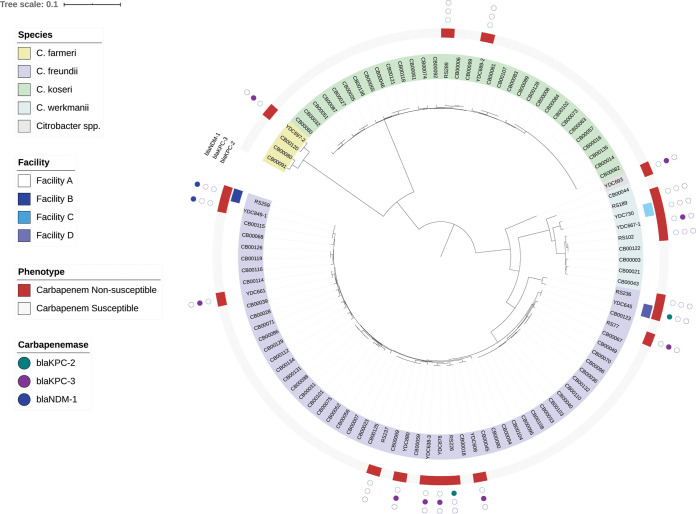
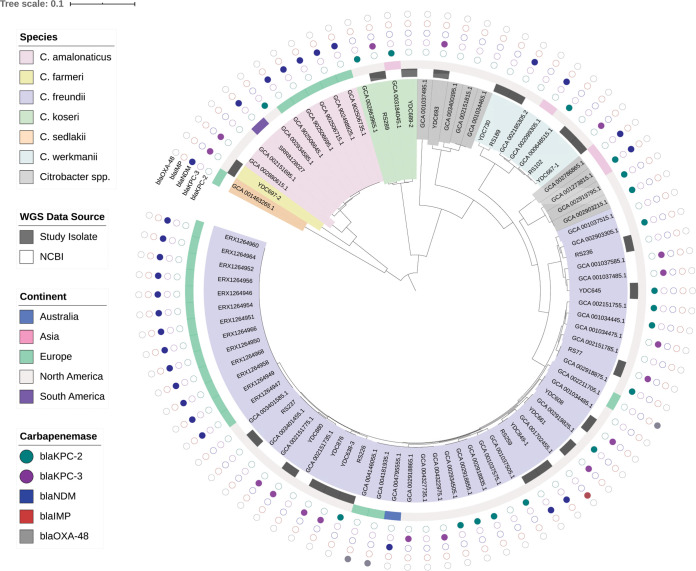
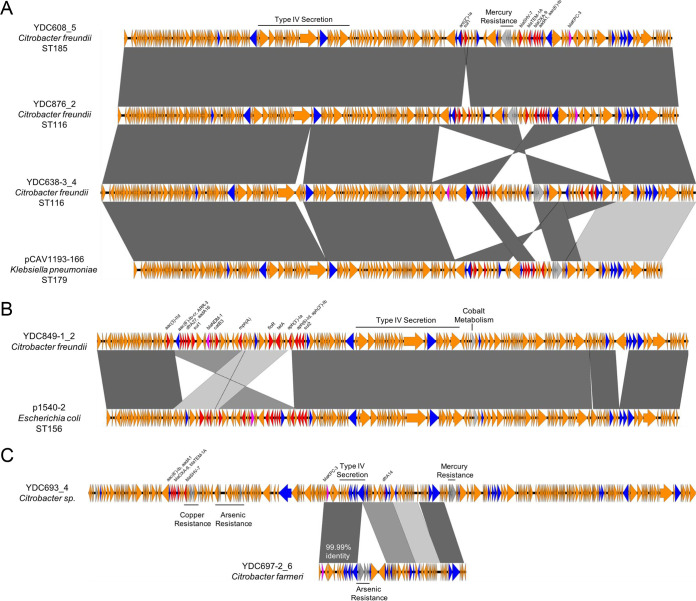
Carbapenem-nonsusceptible Citrobacter spp. (CNSC) are increasingly recognized as health care-associated pathogens. Information regarding their clinical epidemiology, genetic diversity, and mechanisms of carbapenem resistance is lacking. We examined microbiology records of adult patients at the University of Pittsburgh Medical Center (UMPC) Presbyterian Hospital (PUH) from 2000 to 2018 for CNSC, as defined by ertapenem nonsusceptibility. Over this time frame, the proportion of CNSC increased from 4% to 10% (P = 0.03), as did daily defined carbapenem doses/1,000 patient days (6.52 to 34.5; R2 = 0.831; P < 0.001), which correlated with the observed increase in CNSC (lag = 0 years; R2 = 0.660). Twenty CNSC isolates from 19 patients at PUH and other UPMC hospitals were available for further analysis, including whole-genome short-read sequencing and additional antimicrobial susceptibility testing. Of the 19 patients, nearly all acquired CNSC in the health care setting and over half had polymicrobial cultures containing at least one other organism. Among the 20 CNSC isolates, Citrobacter freundii was the predominant species identified (60%). CNSC genomes were compared with genomes of carbapenem-susceptible Citrobacter spp. from UPMC and with other publicly available CNSC genomes. Isolates carrying genes encoding carbapenemases (blaKPC-2,blaKPC-3, and blaNDM-1) were also long-read sequenced, and their carbapenemase-encoding plasmid sequences were compared with one another and with publicly available sequences. Phylogenetic analysis of 102 UPMC Citrobacter genomes showed that CNSC from our setting did not cluster together. Similarly, a global phylogeny of 64 CNSC genomes showed a diverse population structure. Our findings suggest that both local and global CNSC populations are genetically diverse and that CNSC harbor carbapenemase-encoding plasmids found in other Enterobacterales.
Keywords: Citrobacter; carbapenem; carbapenemase; multidrug resistance.
Copyright © 2020 Babiker et al.
Figures

References
-
- Kadri SS, Lai YL, Ricotta EE, Strich JR, Babiker A, Rhee C, Klompas M, Dekker JP, Powers JH III, Danner RL, Adjemian J. 2019. External validation of difficult-to-treat resistance prevalence and mortality risk in Gram-negative bloodstream infection using electronic health record data from 140 US hospitals. Open Forum Infect Dis 6:ofz110. doi: 10.1093/ofid/ofz110. - DOI - PMC - PubMed
-
- WHO. 2017. Global priority list of antibiotic-resistant bacteria to guide research, discover, and development of new antibiotics. World Health Organization, Geneva, Switzerland.
-
- CDC. 2019. Antibiotic resistance threats in the United States. U.S. Department of Health and Human Services, CDC, Atlanta, GA.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
