

Chronic immune checkpoint inhibitor pneumonitis
- PMID: 32554618
- PMCID: PMC7304886
- DOI: 10.1136/jitc-2020-000840
Chronic immune checkpoint inhibitor pneumonitis
Erratum in
-
Correction: Chronic immune checkpoint inhibitor pneumonitis.J Immunother Cancer. 2020 Nov;8(2):e000840corr1. doi: 10.1136/jitc-2020-000840corr1. J Immunother Cancer. 2020. PMID: 33188039 Free PMC article. No abstract available.
Abstract
Background: Pneumonitis from immune checkpoint inhibitors (ICI) is a potentially fatal immune-related adverse event (irAE) from antiprogrammed death 1/programmed death ligand 1 immunotherapy. Most cases of ICI pneumonitis improve or resolve with 4-6 weeks of corticosteroid therapy. Herein, we report the incidence, clinicopathological features and management of patients with non-small cell lung cancer (NSCLC) and melanoma who developed chronic ICI pneumonitis that warrants ≥12 weeks of immunosuppression.
Methods: Patients with ICI pneumonitis were identified from institutional databases of ICI-treated patients with advanced melanoma and NSCLC between January 2011 and July 2018. ICI pneumonitis was defined as clinical/radiographic evidence of lung inflammation without alternative diagnoses, adjudicated by a multidisciplinary team. Chronic ICI pneumonitis was defined as pneumonitis that persists or worsens with steroid tapering, and necessitates ≥12 weeks of immunosuppression, after ICI discontinuation. Serial chest CT was used to assess radiological features, and tumor response by Response EvaluationCriteria for Solid Tumors V.1.1. Bronchoalveolar lavage fluid (BALF) samples were assessed by cell differential. Lung biopsy samples were evaluated by H&E staining and multiplex immunofluorescence (mIF), where available.
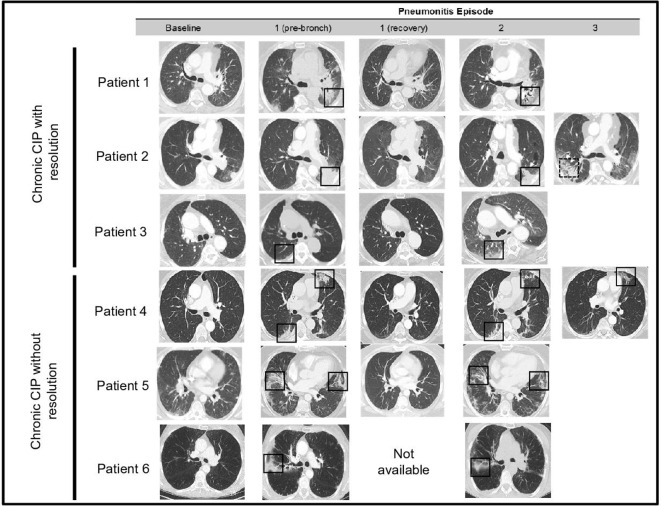
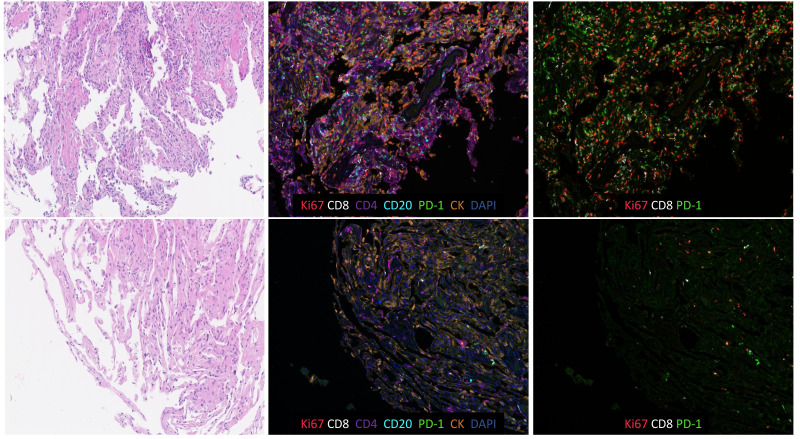
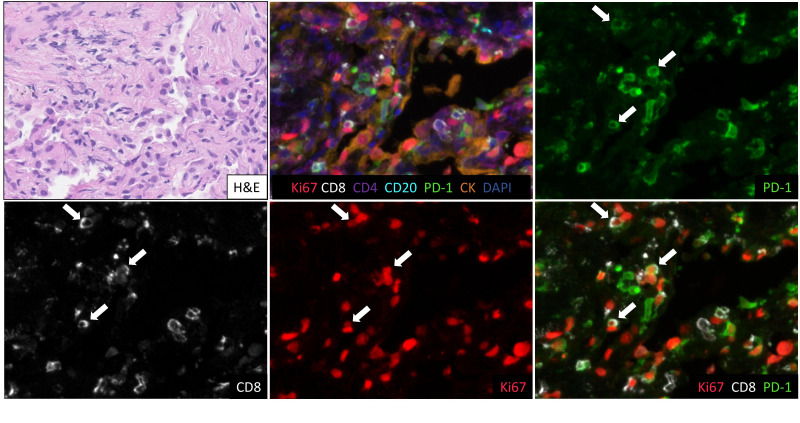
Results: Among 299 patients, 44 developed ICI pneumonitis (NSCLC: 5/205; melanoma: 1/94), and of these, 6 experienced chronic ICI pneumonitis. The overall incidence of chronic ICI pneumonitis was thus 2%. Of those who developed chronic ICI pneumonitis: the majority had NSCLC (5/6), all sustained disease control from ICIs, and none had other concurrent irAEs. Timing of chronic ICI pneumonitis development was variable (range: 0-50 months), and occurred at a median of 12 months post ICI start. Recrudescence of ICI pneumonitis occurred at a median of 6 weeks after initial steroid start (range: 3-12 weeks), with all patients requiring steroid reintroduction when tapered to ≤10 mg prednisone/equivalent. The median total duration of steroids was 37 weeks (range: 16-43+weeks). Re-emergence of radiographic ICI pneumonitis occurred in the same locations on chest CT, in most cases (5/6). All patients who developed chronic ICI pneumonitis had BALF lymphocytosis on cell differential and organising pneumonia on lung biopsy at initial ICI pneumonitis presentation, with persistent BALF lymphocytosis and brisk CD8+ infiltration on mIF at pneumonitis re-emergence during steroid taper.
Conclusions: A subset of patients who develop pneumonitis from ICIs will develop chronic ICI pneumonitis, that warrants long-term immunosuppression of ≥12 weeks, and has distinct clinicopathological features.
Keywords: inflammation; lung neoplasms; melanoma; programmed cell death 1 receptor.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JN: research funding: AstraZeneca, Merck, Consulting/Advisory Board: AstraZeneca, Merck, Bristol-Myers Squibb, Honoraria: AstraZeneca, Merck, Bristol-Myers Squibb. EL: research funding: Bristol-Myers Squibb, Merck, Regeneron, Consulting/Advisory Board: Bristol-Myers Squibb, Merck, Novartis, EMD Serono, Array BioPharma, MacroGenics, Sanofi. PMF: research funding: AstraZeneca, Bristol-Myers Squibb, Corvus, Kyowa, Novartis, Consulting/Advisory Board: AstraZeneca, Bristol-Myers Squibb, Janssen, Merck, Novartis, Lilly, Boehringer. LBY: research funding: Rocket Medical, Consulting/Advisory Board: Boston Scientific. HL: Consulting/Advisory Board: Boston Scientific; DFK/Advisory Board: Consulting: Boston Scientific. JT: research funding: Bristol-Myers Squibb, Consulting/Advisory Board: Bristol-Myers Squibb, Merck, AstraZeneca. JRB: research funding: Bristol-Myers Squibb, Consulting/Advisory Board: Bristol-Myers Squibb, Merck, AstraZeneca, and Genentech, and reports receiving commercial.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous