

Mortality and Recovery Associated with Kidney Failure due to Acute Kidney Injury
- PMID: 32554731
- PMCID: PMC7341787
- DOI: 10.2215/CJN.11200919
Mortality and Recovery Associated with Kidney Failure due to Acute Kidney Injury
Abstract
Background and objectives: AKI requiring dialysis is a contributor to the growing burden of kidney failure, yet little is known about the frequency and patterns of recovery of AKI and its effect on outcomes in patients on incident dialysis.
Design, setting, participants, & measurements: Using the US Renal Data System, we evaluated a cohort of 1,045,540 patients on incident dialysis from January 1, 2005 to December 31, 2014, retrospectively. We examined the association of kidney failure due to AKI with the outcome of all-cause mortality and the associations of sex and race with kidney recovery.
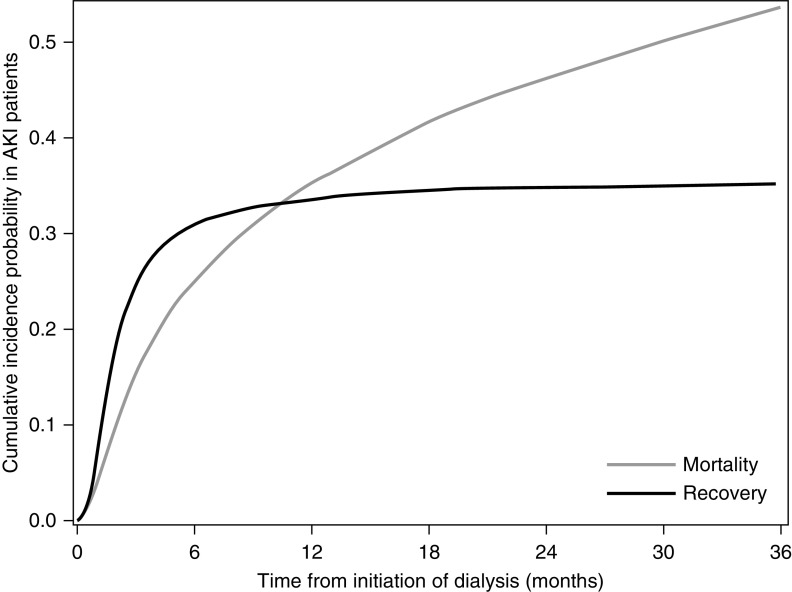
Results: Mean age was 63±15 years, and 32,598 (3%) patients on incident dialysis had kidney failure due to AKI. Compared with kidney failure due to diabetes mellitus, kidney failure attributed to AKI was associated with a higher mortality in the first 0-3 months following dialysis initiation (adjusted hazard ratio, 1.28; 95% confidence interval, 1.24 to 1.32) and 3-6 months (adjusted hazard ratio, 1.16; 95% confidence interval, 1.11 to 1.20). Of the patients with kidney failure due to AKI, 11,498 (35%) eventually recovered their kidney function, 95% of those within 12 months. Women had a lower likelihood of kidney recovery than men (adjusted hazard ratio, 0.86; 95% confidence interval, 0.83 to 0.90). Compared with whites, blacks (adjusted hazard ratio, 0.68; 95% confidence interval, 0.64 to 0.72), Asians (adjusted hazard ratio, 0.82; 95% confidence interval, 0.69 to 0.96), Hispanics (adjusted hazard ratio, 0.82; 95% confidence interval, 0.76 to 0.89), and Native Americans (adjusted hazard ratio, 0.72; 95% confidence interval, 0.54 to 0.95) had lower likelihoods of kidney recovery.
Conclusions: Kidney failure due to AKI confers a higher risk of mortality in the first 6 months compared with kidney failure due to diabetes or other causes. Recovery within 12 months is common, although less so among women than men and among black, Asian, Hispanic, and Native American patients than white patients.
Keywords: Acute Kidney Injury; Asian Continental Ancestry Group; ESKD; Hispanic Americans; acute renal failure; diabetes mellitus; dialysis; kidney; mortality; race; renal recovery; sex.
Copyright © 2020 by the American Society of Nephrology.
Figures




References
-
- Lok CE, Foley R: Vascular access morbidity and mortality: Trends of the last decade. Clin J Am Soc Nephrol 8: 1213–1219, 2013. - PubMed
-
- de Jager DJ, Grootendorst DC, Jager KJ, van Dijk PC, Tomas LM, Ansell D, Collart F, Finne P, Heaf JG, De Meester J, Wetzels JF, Rosendaal FR, Dekker FW: Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA 302: 1782–1789, 2009. - PubMed
-
- US Renal Data System : 2015 Researcher’s Guide to the USRDS Database, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2015
-
- US Department of Health & Human Services: HHS Launches President Trump’s ‘Advancing American Kidney Health’ Initiative, 2019. Available at: https://www.hhs.gov/about/news/2019/07/10/hhs-launches-president-trump-a.... Accessed August 6, 2019
-
- Heung M, Steffick DE, Zivin K, Gillespie BW, Banerjee T, Hsu CY, Powe NR, Pavkov ME, Williams DE, Saran R, Shahinian VB; Centers for Disease Control and Prevention CKD Surveillance Team : Acute kidney injury recovery pattern and subsequent risk of CKD: An analysis of veterans health administration data. Am J Kidney Dis 67: 742–752, 2016. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
