

Comorbidity is associated with disease activity in MS: Findings from the CombiRx trial
- PMID: 32554770
- PMCID: PMC9629214
- DOI: 10.1212/WNL.0000000000010024
Comorbidity is associated with disease activity in MS: Findings from the CombiRx trial
Abstract
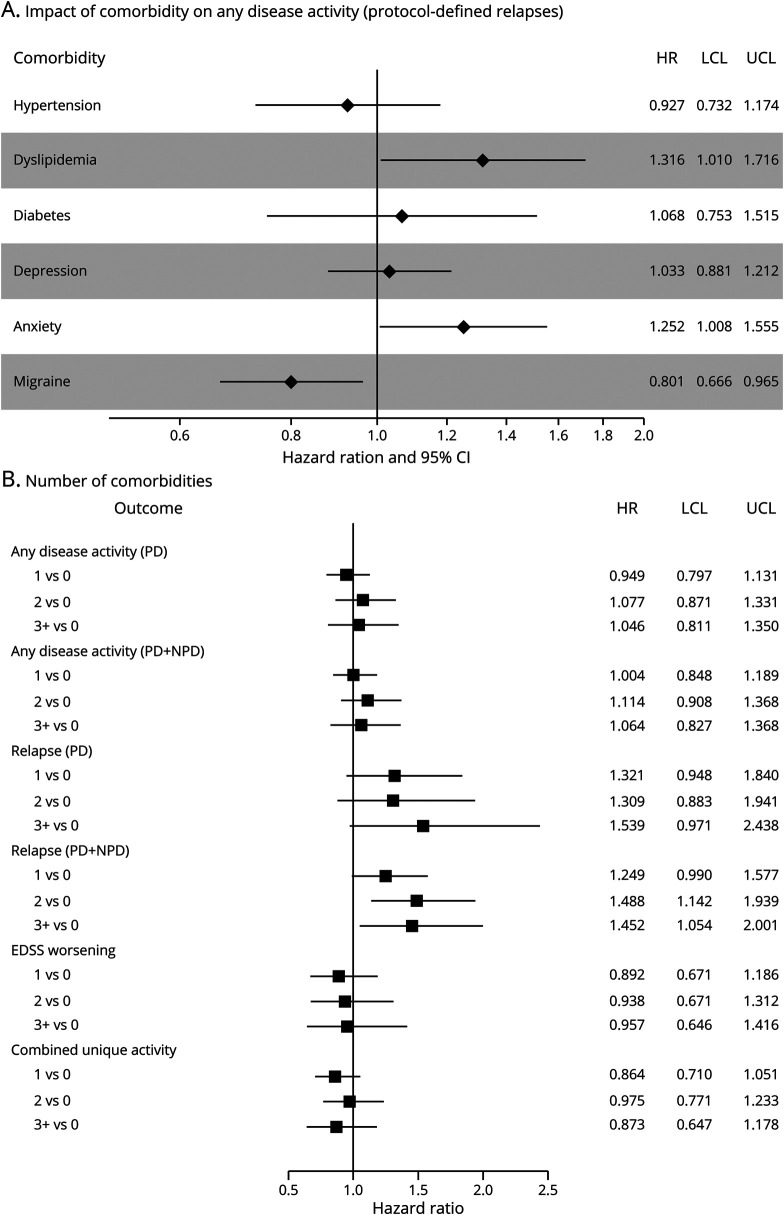
Objective: To determine whether comorbidity is associated with clinical (relapses, disability worsening) and MRI outcomes in multiple sclerosis (MS) by conducting a secondary analysis of the CombiRx clinical trial.
Methods: CombiRx compared interferon beta-1a, glatiramer acetate, and the combination of these agents. For participants eligible for evaluation of 6-month confirmed disability worsening, we used medical history, concomitant medications, and adverse events to ascertain comorbidity status. Comorbid conditions evaluated included hypertension, dyslipidemia, diabetes mellitus, depression, anxiety disorders, and migraine. Clinical outcomes included disease activity consisting of protocol-defined relapses, disability worsening, and MRI activity. We summarized the prevalence of these comorbid conditions and their association with disease activity and its components using multivariable Cox regression.
Results: Of the 1,008 participants randomized, 959 (95.1%) were eligible for assessment of 6-month disability worsening; for this subgroup, the median length of follow-up was 3.4 years (range 0.5-6.9 years). Overall, 55.1% of participants had ≥1 comorbidity at enrollment. After adjustment, anxiety (hazard ratio [HR] 1.25, 95% confidence interval [CI] 1.01-1.55) and dyslipidemia (HR 1.32, 95% CI 1.01-1.72) were associated with an increased hazard of any disease activity, while migraine (HR 0.80, 95% CI 0.67-0.97) was associated with a decreased hazard.
Conclusions: In this large trial population with rigorously obtained outcomes, comorbid conditions were common among participants and influenced disease outcomes, including relapses. The comorbidity burden of clinical trial participants with MS may be an important factor in the outcome of clinical trials. Additional investigations of the impact of comorbidity on clinical trial outcomes and response to disease-modifying therapies are warranted.
Trial registration: ClinicalTrials.gov NCT00211887.
© 2020 American Academy of Neurology.
Figures
Comment in
-
Two decades of research: Time to incorporate comorbidity management into the care of MS?Neurology. 2020 Aug 4;95(5):193-194. doi: 10.1212/WNL.0000000000010036. Epub 2020 Jun 17. Neurology. 2020. PMID: 32554769 No abstract available.
References
-
- Marrie R, Horwitz R, Cutter G, et al. Comorbidity, socioeconomic status and multiple sclerosis. Mult Scler 2008;14:1091–1098. - PubMed
-
- Zhang Y, Zhou Y, van der Mei IAF, et al. Lipid-related genetic polymorphisms significantly modulate the association between lipids and disability progression in multiple sclerosis. J Neurol Neurosurg Psychiatry 2019;90:636–641. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical