

Survival Without Major Morbidity Among Very Low Birth Weight Infants in California
- PMID: 32554813
- PMCID: PMC7329260
- DOI: 10.1542/peds.2019-3865
Survival Without Major Morbidity Among Very Low Birth Weight Infants in California
Abstract
Objectives: To examine trends in survival without major morbidity and its individual components among very low birth weight infants across California and assess remaining gaps that may be opportune targets for improvement efforts.
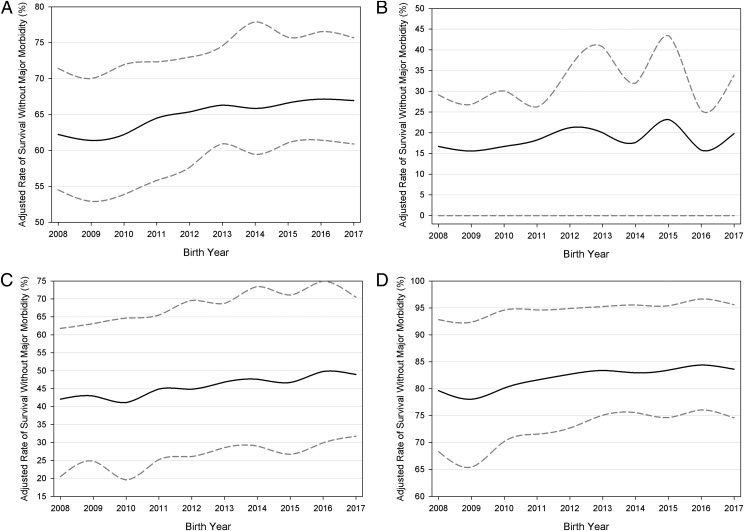
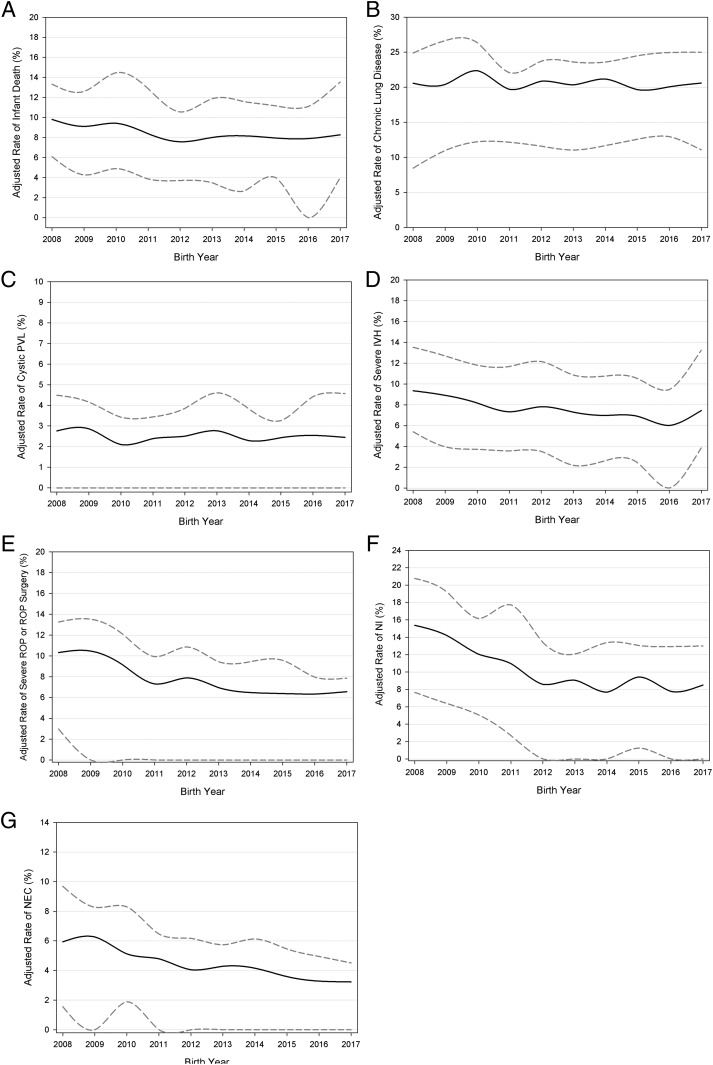
Methods: The study population included infants born between 2008 and 2017 with birth weights of 401 to 1500 g or a gestational age of 22 to 29 weeks. Risk-adjusted trends of survival without major morbidity and its individual components were analyzed. Survival without major morbidity was defined as the absence of death during birth hospitalization, chronic lung disease, severe peri-intraventricular hemorrhage, nosocomial infection, necrotizing enterocolitis, severe retinopathy of prematurity or related surgery, and cystic periventricular leukomalacia. Variations in adjusted rates and/or interquartile ranges were examined. To assess opportunities for additional improvement, all hospitals were reassigned to perform as if in the top quartile, and recalculation of predicted numbers were used to estimate potential benefit.
Results: In this cohort of 49 333 infants across 142 hospitals, survival without major morbidity consistently increased from 62.2% to 66.9% from 2008 to 2017. Network variation decreased, with interquartile ranges decreasing from 21.1% to 19.2%. The largest improvements were seen for necrotizing enterocolitis and nosocomial infection. Bronchopulmonary dysplasia rates did not change significantly. Over the final 3 years, if all hospitals performed as well as the top quartile, an additional 621 infants per year would have survived without major morbidity, accounting for an additional 6.6% annual improvement.
Conclusions: Although trends are promising, bronchopulmonary dysplasia remains a common and persistent major morbidity, remaining a target for continued quality-improvement efforts.
Copyright © 2020 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Comment in
-
Continually Improving Outcomes for Very Low Birth Weight Infants.Pediatrics. 2020 Jul;146(1):e20200436. doi: 10.1542/peds.2020-0436. Epub 2020 Jun 18. Pediatrics. 2020. PMID: 32554812 No abstract available.
References
-
- Payne NR, Finkelstein MJ, Liu M, Kaempf JW, Sharek PJ, Olsen S. NICU practices and outcomes associated with 9 years of quality improvement collaboratives. Pediatrics. 2010;125(3):437–446 - PubMed
-
- Stoll BJ, Hansen N. Infections in VLBW infants: studies from the NICHD Neonatal Research Network. Semin Perinatol. 2003;27(4):293–301 - PubMed
-
- Horbar JD, Carpenter JH, Badger GJ, et al. Mortality and neonatal morbidity among infants 501 to 1500 grams from 2000 to 2009. Pediatrics. 2012;129(6):1019–1026 - PubMed
-
- Horbar JD, Rogowski J, Plsek PE, et al. ; NIC/Q Project Investigators of the Vermont Oxford Network . Collaborative quality improvement for neonatal intensive care. Pediatrics. 2001;107(1):14–22 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
