

Plasma cell-free DNA predicts pediatric cerebral malaria severity
- PMID: 32554925
- PMCID: PMC7406267
- DOI: 10.1172/jci.insight.136279
Plasma cell-free DNA predicts pediatric cerebral malaria severity
Abstract
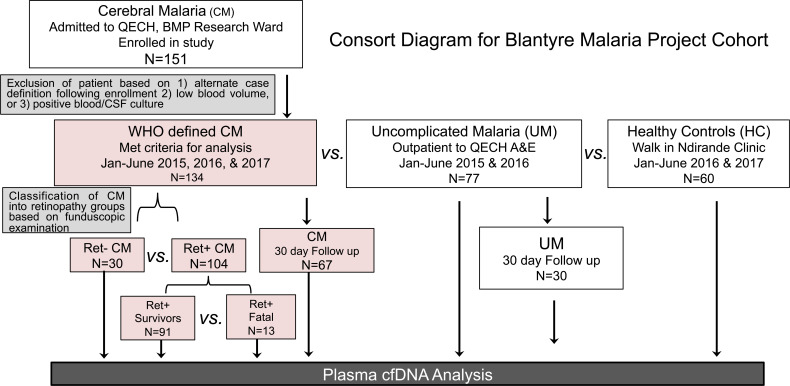
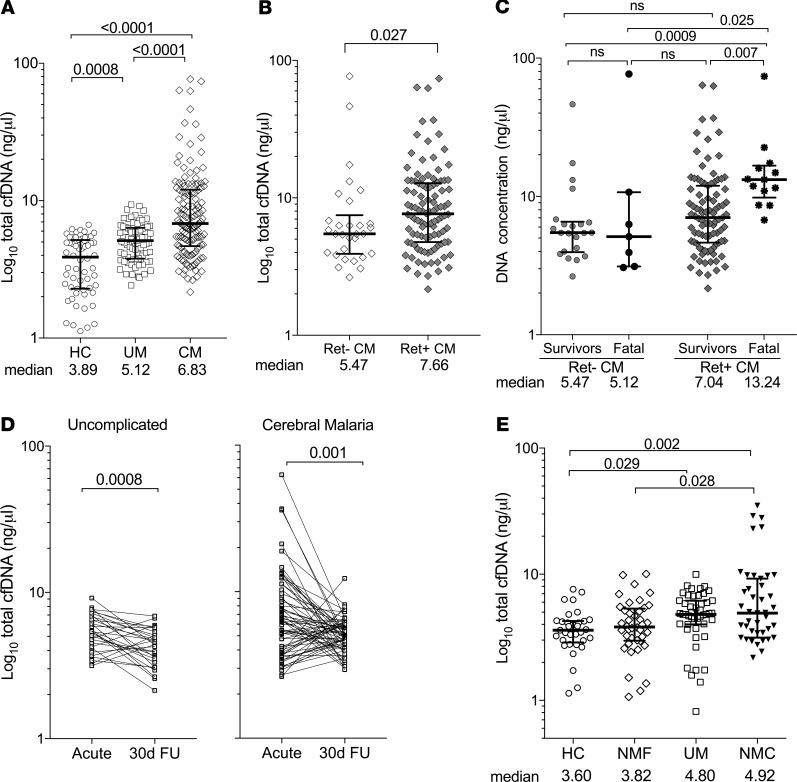
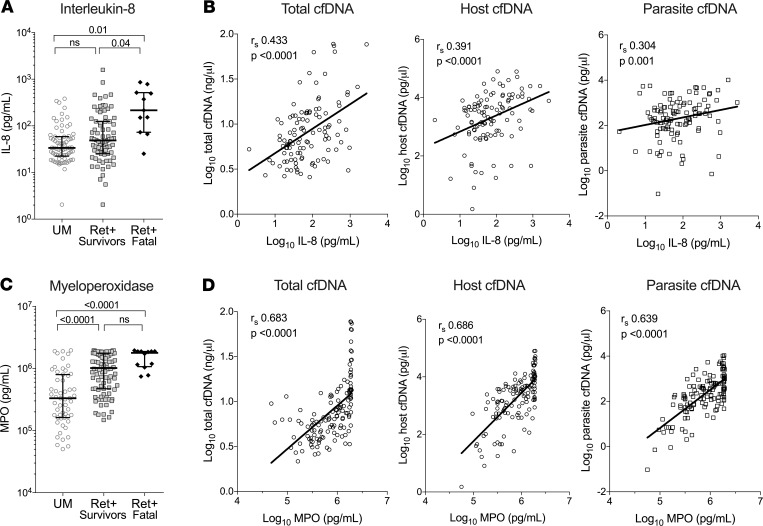
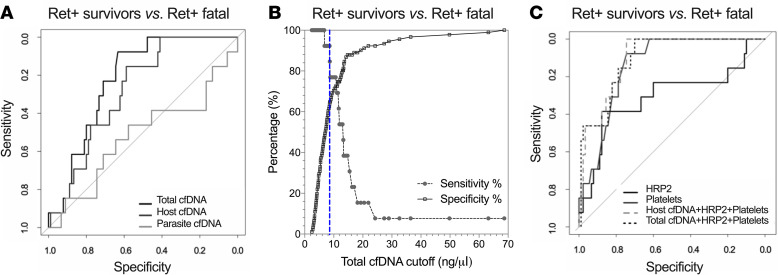
BACKGROUNDPrediction of adverse outcomes in cerebral malaria (CM) is difficult. We hypothesized that cell-free DNA (cfDNA) levels would facilitate identification of severe and potentially fatal CM cases.METHODSIn this retrospective study, plasma from Malawian children with CM (n = 134), uncomplicated malaria (UM, n = 77), and healthy controls (HC, n = 60) was assayed for cfDNA using a fluorescence assay. Host and parasite cfDNA was measured by quantitative PCR. Immune markers were determined by ELISA, Luminex, or cytometric bead array.RESULTSTotal cfDNA increased with malaria severity (HC versus UM, P < 0.001; HC versus CM, P < 0.0001; UM versus CM, P < 0.0001), was elevated in retinopathy-positive (Ret+) CM relative to Ret- CM (7.66 versus 5.47 ng/μL, P = 0.027), and differentiated Ret+ fatal cases from survivors (AUC 0.779; P < 0.001). cfDNA levels in patients with non-malarial febrile illness (NMF, P = 0.25) and non-malarial coma (NMC, P = 0.99) were comparable with UM. Host DNA, rather than parasite DNA, was the major cfDNA contributor (UM, 268 versus 67 pg/μL; CM, 2824 versus 463 pg/μL). Host and parasite cfDNA distinguished CM by retinopathy (host, AUC 0.715, P = 0.0001; parasite, AUC 0.745, P = 0.0001), but only host cfDNA distinguished fatal cases (AUC 0.715, P = 0.0001). Total cfDNA correlated with neutrophil markers IL-8 (rs = 0.433, P < 0.0001) and myeloperoxidase (rs = 0.683, P < 0.0001).CONCLUSIONQuantifying plasma cfDNA is a simple assay useful in identifying children at risk for fatal outcome and has promise as a point-of-care assay. Elevated cfDNA suggests a link with host inflammatory pathways in fatal CM.FUNDINGNIH NCATS (AK), Burroughs-Wellcome (AK), and National Health and Medical Research Council of Australia (SJR).
Keywords: Infectious disease; Inflammation; Malaria.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
