

The senescence-associated secretome as an indicator of age and medical risk
- PMID: 32554926
- PMCID: PMC7406245
- DOI: 10.1172/jci.insight.133668
The senescence-associated secretome as an indicator of age and medical risk
Abstract
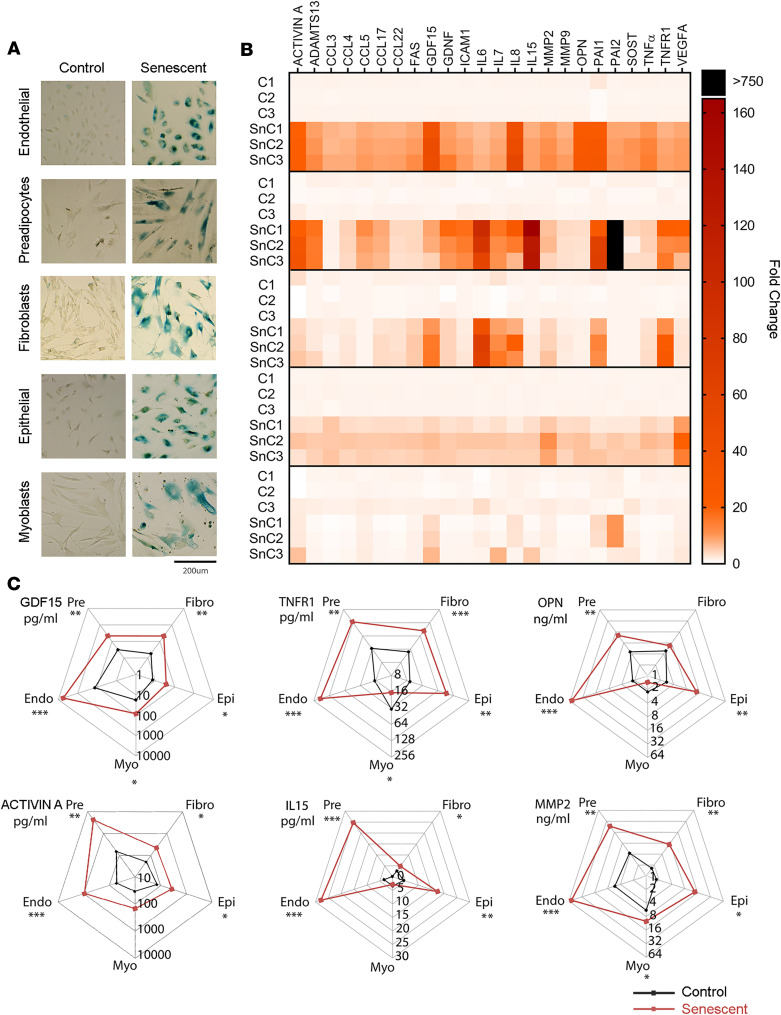
Produced by senescent cells, the senescence-associated secretory phenotype (SASP) is a potential driver of age-related dysfunction. We tested whether circulating concentrations of SASP proteins reflect age and medical risk in humans. We first screened senescent endothelial cells, fibroblasts, preadipocytes, epithelial cells, and myoblasts to identify candidates for human profiling. We then tested associations between circulating SASP proteins and clinical data from individuals throughout the life span and older adults undergoing surgery for prevalent but distinct age-related diseases. A community-based sample of people aged 20-90 years (retrospective cross-sectional) was studied to test associations between circulating SASP factors and chronological age. A subset of this cohort aged 60-90 years and separate cohorts of older adults undergoing surgery for severe aortic stenosis (prospective longitudinal) or ovarian cancer (prospective case-control) were studied to assess relationships between circulating concentrations of SASP proteins and biological age (determined by the accumulation of age-related health deficits) and/or postsurgical outcomes. We showed that SASP proteins were positively associated with age, frailty, and adverse postsurgery outcomes. A panel of 7 SASP factors composed of growth differentiation factor 15 (GDF15), TNF receptor superfamily member 6 (FAS), osteopontin (OPN), TNF receptor 1 (TNFR1), ACTIVIN A, chemokine (C-C motif) ligand 3 (CCL3), and IL-15 predicted adverse events markedly better than a single SASP protein or age. Our findings suggest that the circulating SASP may serve as a clinically useful candidate biomarker of age-related health and a powerful tool for interventional human studies.
Keywords: Aging; Cellular senescence.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
