

Hypermobility of the First Ray: the Cinderella of the measurements conventionally assessed for correction of Hallux Valgus
- PMID: 32555076
- PMCID: PMC7944838
- DOI: 10.23750/abm.v91i4-S.9769
Hypermobility of the First Ray: the Cinderella of the measurements conventionally assessed for correction of Hallux Valgus
Abstract
Background and aim of the work: hypermobility of the first ray (FRH) began to be considered as a pathological entity from Morton's studies and was associated as a primary cause of hallux valgus (HV ). Currently, this relationship is in discussion, and various authors consider FRH as a consequence of the deformity. The purpose of this narrative review is to summarise the most influential publications relating to First Ray Mobility (FRM) to increase knowledge and promote its conventional assessment during clinical practice.
Methods: papers of the last century were selected to obtain a homogeneous and up-to-date overview of I-MTCJ mobility and HV, as well as their relationship and management.
Results: in recent years, FRH was studied from a biomechanical and pathophysiologic point of view. There is still not enough data regarding the aetiology of FRM. The higher rate of instability found in HV lacks an explanation of which is the cause and which is the effect. However, the Lapidus arthrodesis is still a valid method in cases of FRH and HV, even if is not rigorously indicated to treat both. When approaching FRH, radiographic or clinical findings are mandatory for the right diagnosis.
Conclusions: FRM is an important factor that must be considered in routine clinical practice and prior and post HV surgery, as much as the conventional parameters assessed. Surgeons should consider performing I-MTCJ arthrodesis only if strictly necessary, also paying attention to soft tissue balancing. Improving the measurement of FRH could be useful to determine if it is a cause or effect of the HV deformity.
Conflict of interest statement
The authors declare that they have no conflict of interest related to the publication of this manuscript, and they have not received benefits or financial funds in support of this study.
Figures



References
-
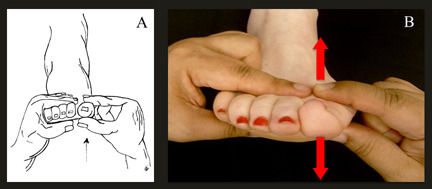
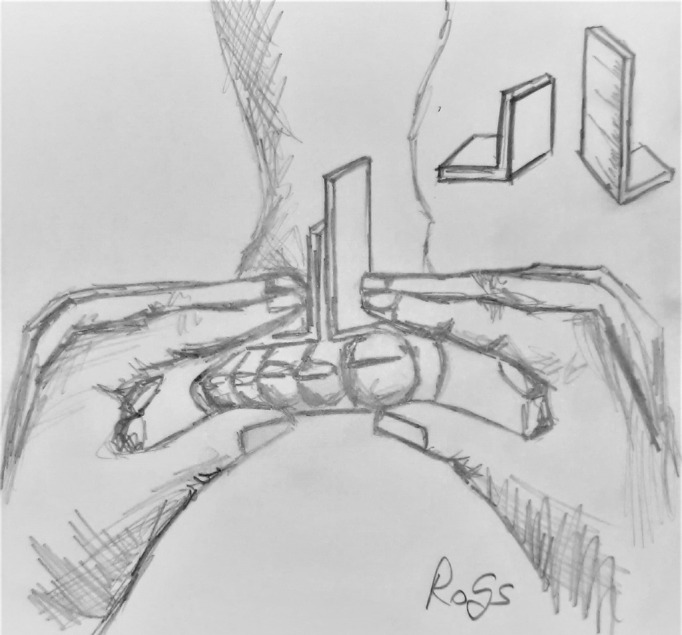
- Voellmicke KV, Deland JT. Manual examination technique to assess dorsal instability of the first ray. Foot ankle Int. 2002 Nov 17;23(11):1040–1. - PubMed
-
- Glasoe WM, Allen MK, Saltzman CL, Ludewig PM, Sublett SH. Comparison of Two Methods Used to Assess First-Ray Mobility. Foot Ankle Int. 2002 Mar 28;23(3):248–52. - PubMed
-
- Morton DJ. Hypermobility of the first metatarsal bone: the interlinking factor between metatarsalgia and longitudinal arch strains. JBJS. 1928;10(2):187–196.
-
- Lapidus PW. The operative correction of the metatarsus primus varus in hallux valgus. Surg Gynecol Obs. 1934:183–91.
-
- Lapidus PW. A quarter of a century of experience with the operative correction of the metatarsus varus primus in hallux valgus. Bull Hosp Joint Dis. 1956 Oct;17(2):404–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
