

Intracellular calcium leak in heart failure and atrial fibrillation: a unifying mechanism and therapeutic target
- PMID: 32555383
- PMCID: PMC8362847
- DOI: 10.1038/s41569-020-0394-8
Intracellular calcium leak in heart failure and atrial fibrillation: a unifying mechanism and therapeutic target
Abstract
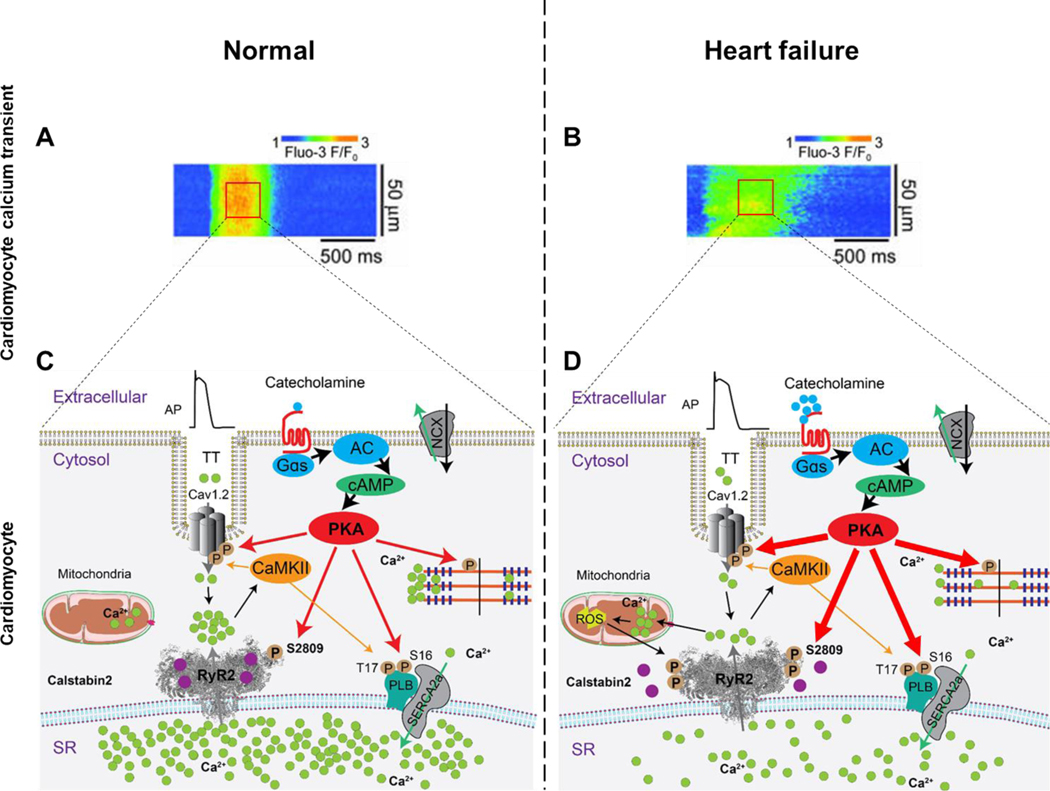
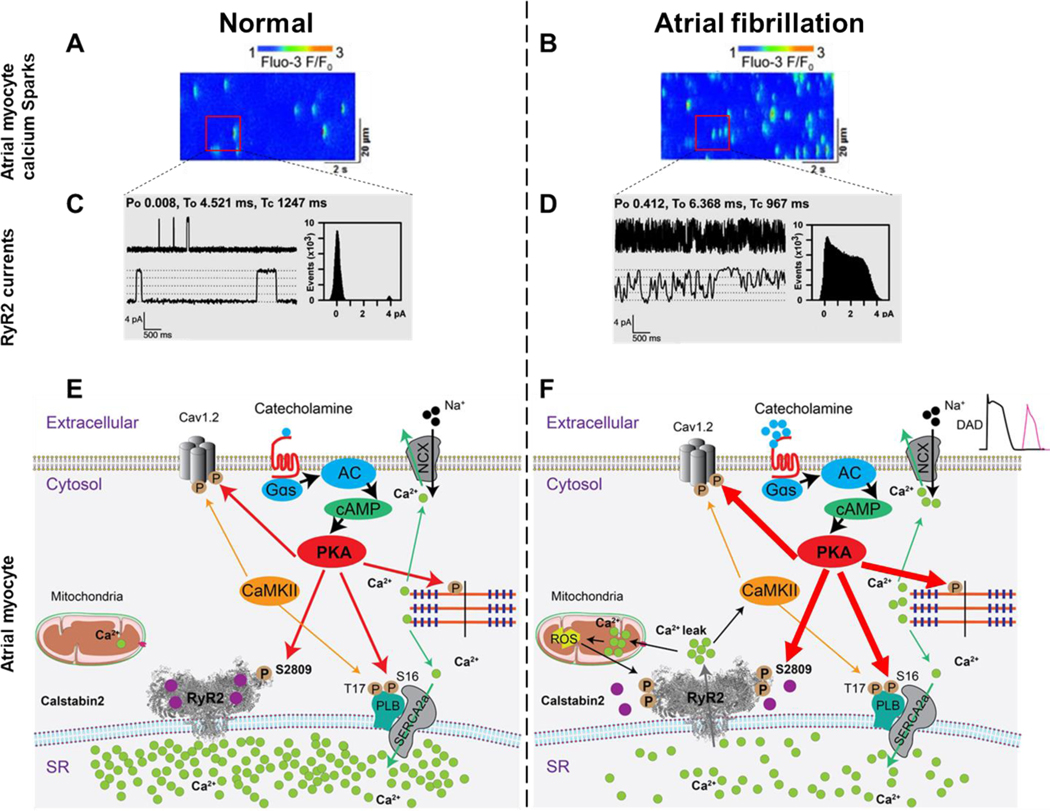
Ca2+ is a fundamental second messenger in all cell types and is required for numerous essential cellular functions, including cardiac and skeletal muscle contraction. The intracellular concentration of free Ca2+ ([Ca2+]) is regulated primarily by ion channels, pumps (ATPases), exchangers and Ca2+-binding proteins. Defective regulation of [Ca2+] is found in a diverse spectrum of pathological states that affect all the major organs. In the heart, abnormalities in the regulation of cytosolic and mitochondrial [Ca2+] occur in heart failure (HF) and atrial fibrillation (AF), two common forms of heart disease and leading contributors to morbidity and mortality. In this Review, we focus on the mechanisms that regulate ryanodine receptor 2 (RYR2), the major sarcoplasmic reticulum (SR) Ca2+-release channel in the heart, how RYR2 becomes dysfunctional in HF and AF, and its potential as a therapeutic target. Inherited RYR2 mutations and/or stress-induced phosphorylation and oxidation of the protein destabilize the closed state of the channel, resulting in a pathological diastolic Ca2+ leak from the SR that both triggers arrhythmias and impairs contractility. On the basis of our increased understanding of SR Ca2+ leak as a shared Ca2+-dependent pathological mechanism in HF and AF, a new class of drugs developed in our laboratory, known as rycals, which stabilize RYR2 channels and prevent Ca2+ leak from the SR, are undergoing investigation in clinical trials.
Figures



Comment in
-
Reply to 'Mechanisms of ryanodine receptor 2 dysfunction in heart failure'.Nat Rev Cardiol. 2020 Nov;17(11):749-750. doi: 10.1038/s41569-020-00444-w. Nat Rev Cardiol. 2020. PMID: 32901149 No abstract available.
-
Mechanisms of ryanodine receptor 2 dysfunction in heart failure.Nat Rev Cardiol. 2020 Nov;17(11):748. doi: 10.1038/s41569-020-00443-x. Nat Rev Cardiol. 2020. PMID: 32901150 No abstract available.
References
-
- Writing Group, M. et al.2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 16, e66–e93, doi:10.1016/j.hrthm.2019.01.024 (2019). - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
