

ISS alone, is not sufficient to correctly assign patients post hoc to trauma team requirement
- PMID: 32556366
- PMCID: PMC8825400
- DOI: 10.1007/s00068-020-01410-4
ISS alone, is not sufficient to correctly assign patients post hoc to trauma team requirement
Abstract
Purpose: An injury severity score (ISS) ≥ 16 alone, is commonly used post hoc to define the correct activation of a trauma team. However, abnormal vital functions and the requirement of life-saving procedures may also have a role in defining trauma team requirement post hoc. The aim of this study was to describe their prevalence and mortality in severely injured patients and to estimate their potential additional value in the definition of trauma team requirement as compared to the definition based on ISS alone.
Methods: Retrospective analysis of a trauma registry including patients with trauma team activation from the years 2009 until 2015, who were 16 years of age or older and were brought to the trauma center directly from the scene. Patients were divided into a group with an ISS ≥ 16 vs. ISS < 16. For analysis a predefined list of abnormal vital functions and life-saving interventions was used.
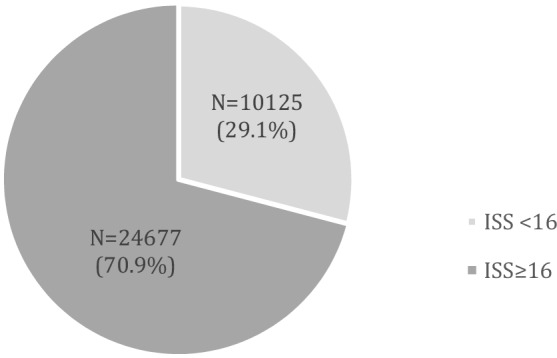
Results: 58,723 patients were included in the study (N = 32,653 with ISS ≥ 16; N = 26,070 with ISS < 16). From the total number of patients that required life-saving procedures or presented with abnormal vital functions 29.1% were found in the ISS < 16 group. From the ISS < 16 group, 36.7% of patients required life-saving procedures or presented with abnormal vital signs. The mortality of those was 8.1%.
Conclusions: Defining the true requirement of trauma team activation post hoc by using ISS ≥ 16 alone does miss a considerable number of subjects who require life-saving interventions or present with abnormal vital functions. Therefore, life-saving interventions and abnormal vital functions should be included in the definitions for trauma team requirement. Further studies have to evaluate, which life-saving procedures and abnormal vital functions are most relevant.
Keywords: Emergency service; Hospital; Quality control; Trauma centers; Trauma team; Trauma team activation; Triage; Wounds and injuries.
© 2020. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Newgard CD, Hsia RY, Mann NC, Schmidt T, Sahni R, Bulger EM, et al. The trade-offs in field trauma triage: a multiregion assessment of accuracy metrics and volume shifts associated with different triage strategies. J Trauma Acute Care Surg. 2013;74:1298–1306. doi: 10.1097/ta.0b013e31828b7848. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
