

Paediatric femur fractures-the value of contextual information on judgement in possible child abuse cases: are we bias?
- PMID: 32556507
- PMCID: PMC7782380
- DOI: 10.1007/s00431-020-03704-6
Paediatric femur fractures-the value of contextual information on judgement in possible child abuse cases: are we bias?
Abstract
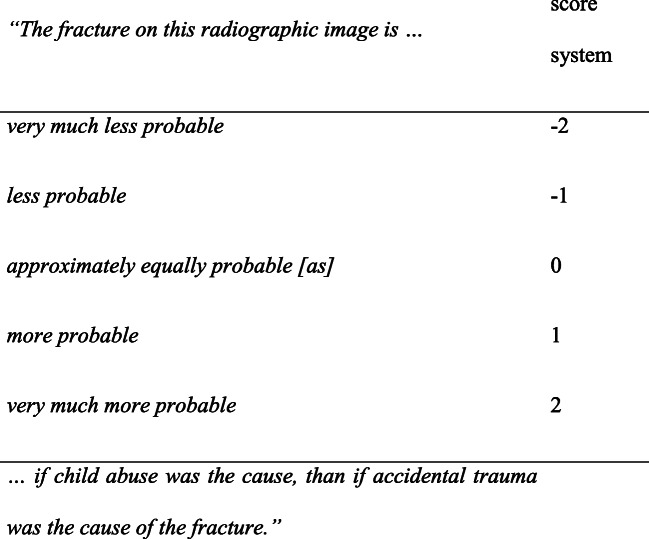
The majority of paediatric femur fractures result from accidental trauma; however, it is important to consider non-accidental trauma, especially in pre-ambulatory children. We study whether irrelevant contextual information subconsciously influences conclusions of healthcare professionals with respect to whether observations provide evidence for non-accidental trauma. A survey with nine radiographs of femur shaft fractures was designed. Two different clinical histories (vignettes) with contextual information were designed, non-abuse versus abuse context. One of both vignettes was randomly assigned to the radiograph shown to the participant, followed by a question with a 5-point answer scale, which represents a verbal expression of the likelihood ratio of the fracture regarding a non-accidental versus accidental cause. Participants were medical residents and staff members of different specialties from several Dutch hospitals. A total of 172 participants responded. The reported evidential strength of the vignettes with a non-abuse context was 0.19 (n = 784; 95%CI 0.10-0.28) and for the abuse context 0.94 (n = 764; 95%CI 0.86-1.02; p < 0.001). Women reported a stronger evidential strength than men, but both were influenced by context. Emergency department and paediatric doctors were more likely to decide that non-accidental trauma was the cause; paediatric radiologists were the least likely. Experience in years of practice and current function did not prevent participants from being bias.Conclusion: This study shows that the interpretation of medical results by healthcare professionals can be influenced by contextual information, such as low income and marital status, which are irrelevant to the decision as to whether abuse might have occurred. Given the same information about an injury, women, emergency department and paediatric doctors were more likely to decide that non-accidental trauma was the cause, while paediatric radiologists were least likely to decide this outcome. It is important to prevent contextual influence as much as possible, by recognizing it and implementing a management contextual information procedure. What is Known: • Contextual information is of possible influence on healthcare professionals in identifying non-accidental trauma. • Increased working experience is thought to be protective against this influence. What is New: • Contextual information influenced the interpretation of medical results by healthcare professionals regardless of work experience. • The interpretation of medical results by healthcare professionals is influenced by both affirmative and negative contextual information.
Keywords: Child abuse; Contextual information; Femur fracture; Influence.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
-
- Flaherty EG, Perez-Rossello JM, Levine MA, Hennrikus WL, American Academy of Pediatrics Committee on Child A, Neglect, Section on Radiology AAoP, Section on Endocrinology AAoP, Section on Orthopaedics AAoP, Society for Pediatric R Evaluating children with fractures for child physical abuse. Pediatrics. 2014;133(2):e477–e489. doi: 10.1542/peds.2013-3793. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
