

SARS-CoV-2 coinfections: Could influenza and the common cold be beneficial?
- PMID: 32557776
- PMCID: PMC7300957
- DOI: 10.1002/jmv.26098
SARS-CoV-2 coinfections: Could influenza and the common cold be beneficial?
Abstract
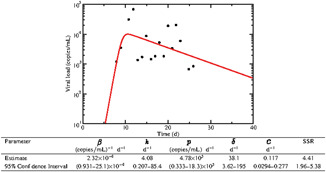
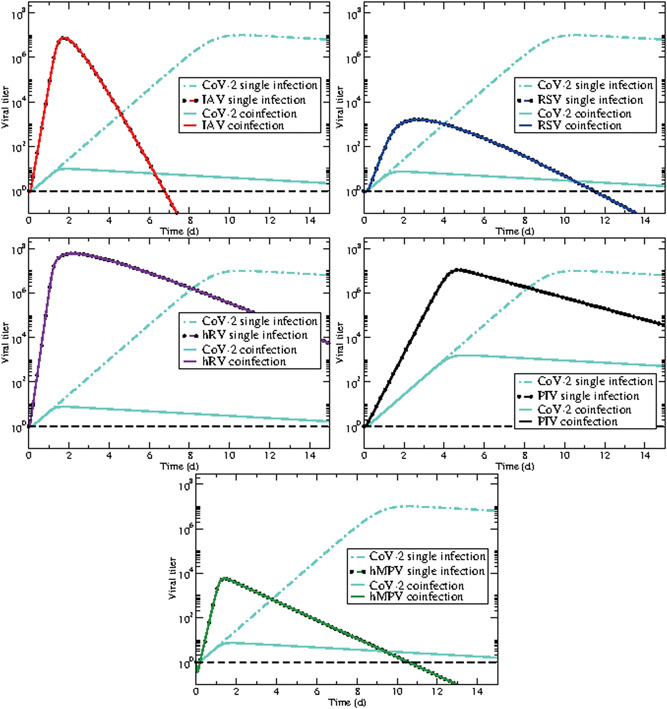
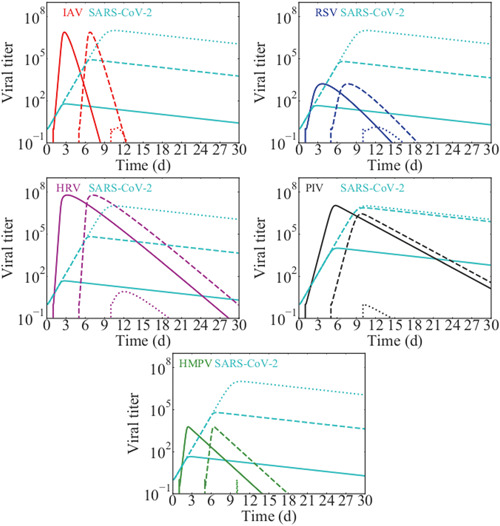
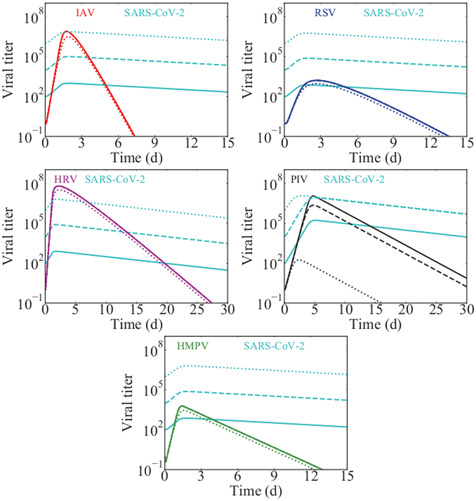
The novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly spread around the world, causing serious illness and death and creating a heavy burden on the healthcare systems of many countries. Since the virus first emerged in late November 2019, its spread has coincided with peak circulation of several seasonal respiratory viruses, yet some studies have noted limited coinfections between SARS-CoV-2 and other viruses. We use a mathematical model of viral coinfection to study SARS-CoV-2 coinfections, finding that SARS-CoV-2 replication is easily suppressed by many common respiratory viruses. According to our model, this suppression is because SARS-CoV-2 has a lower growth rate (1.8/d) than the other viruses examined in this study. The suppression of SARS-CoV-2 by other pathogens could have implications for the timing and severity of a second wave.
Keywords: SARS coronavirus; computer modeling; human metapneumovirus; human rhinovirus; influenza virus; respiratory syncytial virus.
© 2020 Wiley Periodicals LLC.
Figures
References
-
- Govorkova EA, Ilyushina NA, Marathe BM, McClaren JL, Webster RG. Clinical characteristics of covid‐19 in New York City. N Engl J Med. 2020;84:8042‐8050. 10.1128/JVI.00689-10 - DOI
-
- Lai CC, Wang CY, Wang YH, Hsueh SC, Ko WC, Hsueh PR. Global epidemiology of coronavirus disease 2019 (COVID‐19): disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. Int J Antimicrob Agents. 2020;55(4):105946. 10.1016/j.ijantimicag.2020.105946 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
