

Opioid, gabapentinoid, and nonsteroidal anti-inflammatory medication use and the risks of atrial fibrillation and supraventricular ectopy in the Multi-Ethnic Study of Atherosclerosis
- PMID: 32558036
- PMCID: PMC7933496
- DOI: 10.1002/pds.5036
Opioid, gabapentinoid, and nonsteroidal anti-inflammatory medication use and the risks of atrial fibrillation and supraventricular ectopy in the Multi-Ethnic Study of Atherosclerosis
Abstract
Purpose: Opioids, gabapentinoids, and nonsteroidal anti-inflammatory drugs (NSAIDs) may have adverse cardiovascular effects. We evaluated whether these medications were associated with incident clinically detected atrial fibrillation (AF) or monitor-detected supraventricular ectopy (SVE), including premature atrial contractions (PACs) and supraventricular tachycardia (SVT).
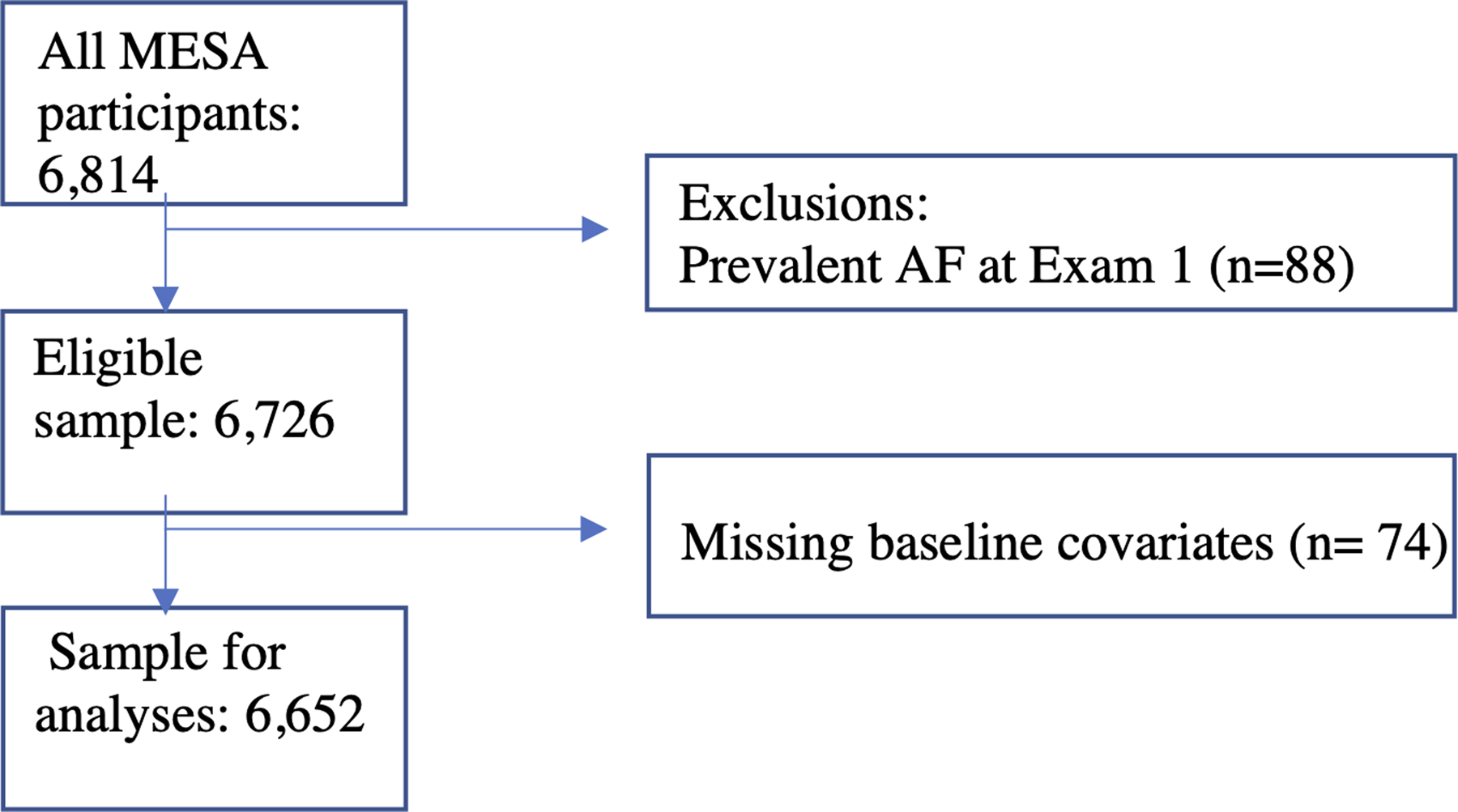
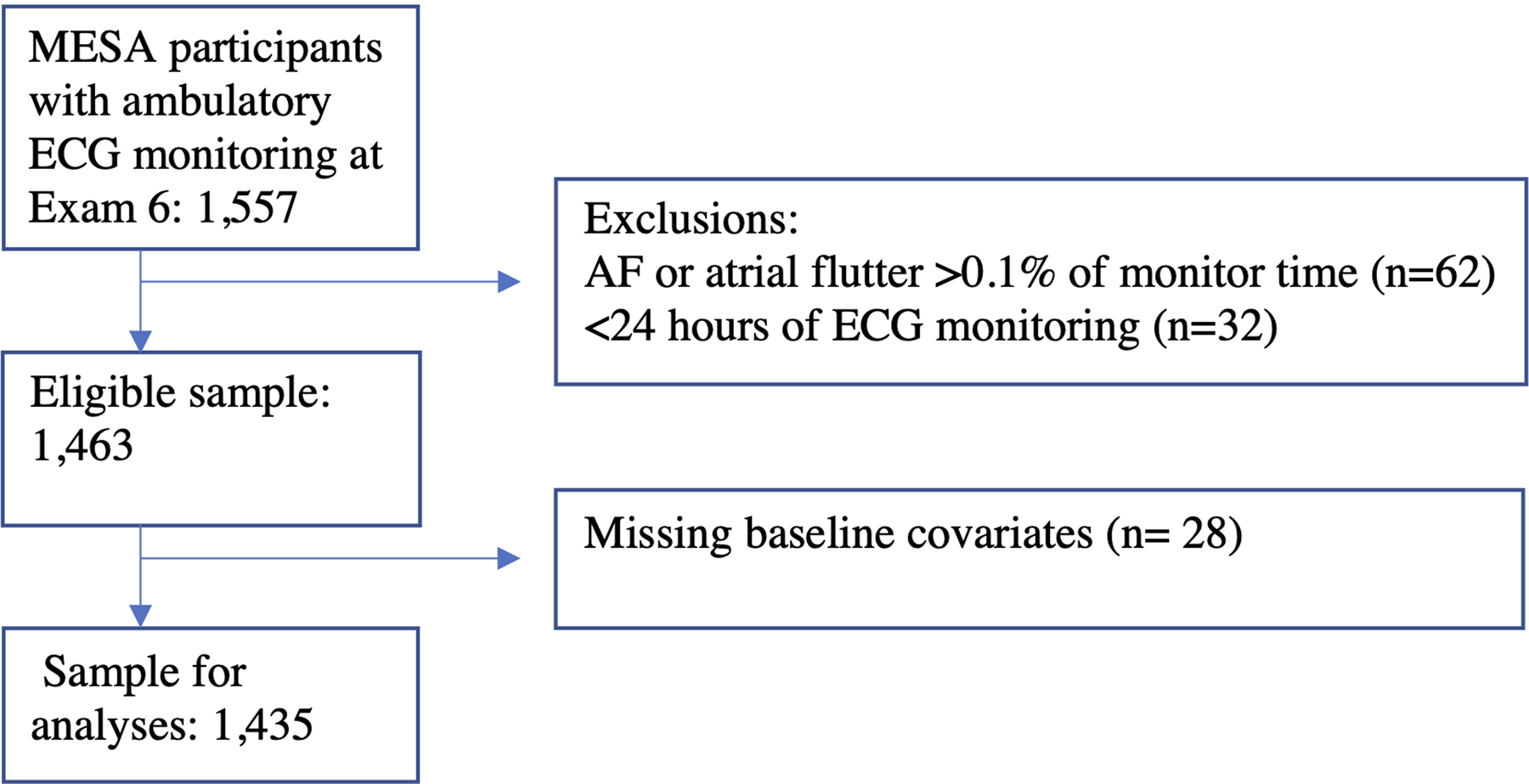
Methods: We used data from the Multi-Ethnic Study of Atherosclerosis (MESA), a cohort study that enrolled 6814 Americans without clinically detected cardiovascular disease in 2000 to 2002. At the 2016 to 2018 examination, 1557 individuals received ambulatory electrocardiographic (ECG) monitoring. Longitudinal analyses investigated time-varying medication exposures at the first five exams (through 2011) in relation to incident clinically detected AF through 2015 using Cox proportional hazards regression models. Cross-sectional analyses investigated medication exposures at 2016 to 2018 examination and the risk of monitor-detected SVE using linear regression models.
Results: The longitudinal cohort included 6652 participants. During 12.4 years of mean follow-up, 982 participants (14.7%) experienced incident clinically detected AF. Use of opioids, gabapentinoids, and NSAIDs were not associated with incident AF. The cross-sectional analysis included 1435 participants with ECG monitoring. Gabapentinoid use was associated with an 84% greater average frequency of PACs/hour (95% CI, 25%-171%) and a 44% greater average number of runs of SVT/day (95% CI, 3%-100%). No associations were found with use of opioids or NSAIDs in cross-sectional analyses.
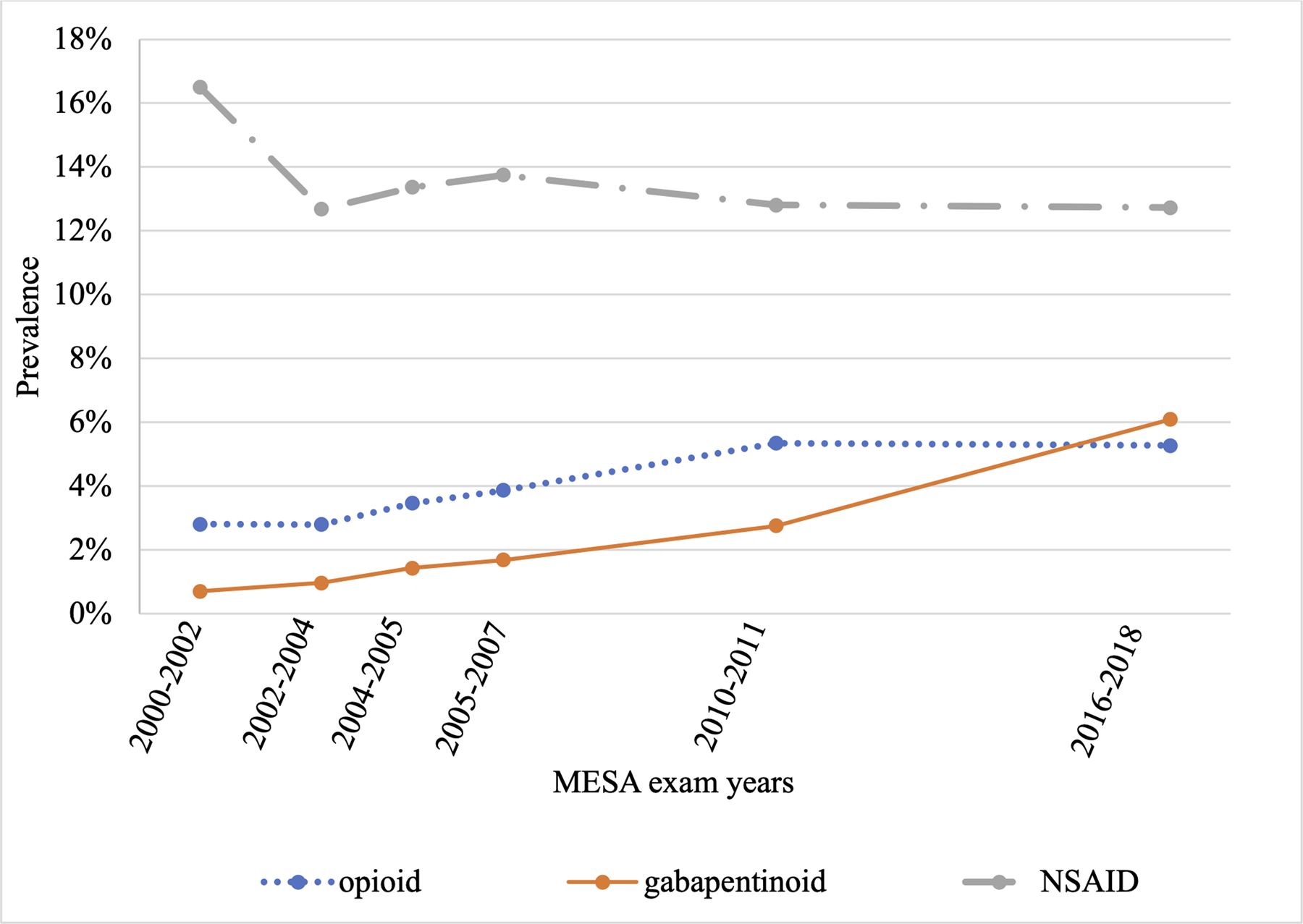
Conclusions: In this study, gabapentinoid use was associated with SVE. Given the rapid increase in gabapentinoid use, additional studies are needed to clarify whether these medications cause cardiovascular complications.
Keywords: arrhythmia; atrial fibrillation; cohort study; gabapentinoid; opioid; pharmacoepidemiology; supraventricular tachycardia.
© 2020 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Centers for Disease C, Prevention. Vital signs: overdoses of prescription opioid pain relievers---United States, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60(43):1487–1492. - PubMed
-
- Goodman CW, Brett AS. Gabapentin and Pregabalin for Pain - Is Increased Prescribing a Cause for Concern? N Engl J Med. 2017;377(5):411–414. - PubMed
-
- Abdulla A, Adams N, Bone M, et al. Guidance on the management of pain in older people. Age Ageing. 2013;42 Suppl 1:i1–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 75N95020D00003/DA/NIDA NIH HHS/United States
- N01-HC-95166/HL/NHLBI NIH HHS/United States
- 75N93020D00002/AI/NIAID NIH HHS/United States
- K08HL116640/HL/NHLBI NIH HHS/United States
- 75N95020D00007/DA/NIDA NIH HHS/United States
- 75N99020D00007/OF/ORFDO NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- 75N90020D00002/CL/CLC NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- N01-HC-95159/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- 75N96020D00002/ES/NIEHS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- UL1-TR-001420/TR/NCATS NIH HHS/United States
- R01HL142599/HL/NHLBI NIH HHS/United States
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- T32 HL007828/HL/NHLBI NIH HHS/United States
- 75N99020D00003/OF/ORFDO NIH HHS/United States
- N01-HC-95160/HL/NHLBI NIH HHS/United States
- 75N95020D00002/DA/NIDA NIH HHS/United States
- N01-HC-95167/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- R01 HL142599/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- K08 HL116640/HL/NHLBI NIH HHS/United States
- 75N90020D00003/CL/CLC NIH HHS/United States
- 75N96020D00003/ES/NIEHS NIH HHS/United States
- N01-HC-95163/HL/NHLBI NIH HHS/United States
- 75N99020D00002/OF/ORFDO NIH HHS/United States
- UL1-TR-001079/TR/NCATS NIH HHS/United States
- N01-HC-95168/HL/NHLBI NIH HHS/United States
- 75N99020D00006/OF/ORFDO NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- 75N95020D00005/DA/NIDA NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- N01-HC-95162/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- N01-HC-95164/HL/NHLBI NIH HHS/United States
- 75N99020D00005/OF/ORFDO NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01-HC-95165/HL/NHLBI NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- 75N98020D00007/OD/NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- R01HL127659/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- 75N95020D00004/DA/NIDA NIH HHS/United States
- R01 HL127659/HL/NHLBI NIH HHS/United States
- 75N99020D00004/OF/ORFDO NIH HHS/United States
- UL1-TR-000040/TR/NCATS NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- T32HL007828/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- N01-HC-95169/HL/NHLBI NIH HHS/United States
- N01-HC-95161/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
