

Economic analysis of screening for subclinical rejection in kidney transplantation using protocol biopsies and noninvasive biomarkers
- PMID: 32558153
- PMCID: PMC7744316
- DOI: 10.1111/ajt.16150
Economic analysis of screening for subclinical rejection in kidney transplantation using protocol biopsies and noninvasive biomarkers
Abstract
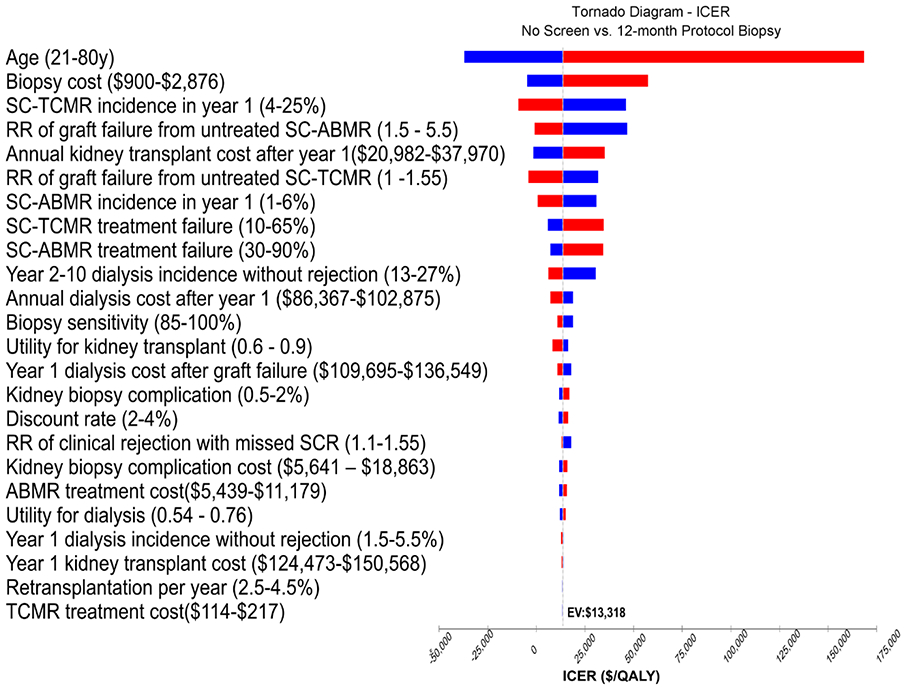
Subclinical rejection (SCR) screening in kidney transplantation (KT) using protocol biopsies and noninvasive biomarkers has not been evaluated from an economic perspective. We assessed cost-effectiveness from the health sector perspective of SCR screening in the first year after KT using a Markov model that compared no screening with screening using protocol biopsy or biomarker at 3 months, 12 months, 3 and 12 months, or 3, 6, and 12 months. We used 12% subclinical cellular rejection and 3% subclinical antibody-mediated rejection (SC-ABMR) for the base-case cohort. Results favored 1-time screening at peak SCR incidence rather than repeated screening. Screening 2 or 3 times was favored only with age <35 years and with high SC-ABMR incidence. Compared to biomarkers, protocol biopsy yielded more quality-adjusted life years (QALYs) at lower cost. A 12-month biopsy cost $13 318/QALY for the base-case cohort. Screening for cellular rejection in the absence of SC-ABMR was less cost effective with 12-month biopsy costing $46 370/QALY. Screening was less cost effective in patients >60 years. Using biomarker twice or thrice was cost effective only if biomarker cost was <$700. In conclusion, in KT, screening for SCR more than once during the first year is not economically reasonable. Screening with protocol biopsy was favored over biomarkers.
Keywords: biomarker; clinical research/practice; economics; health services and outcomes research; kidney transplantation/nephrology; mathematical model; protocol biopsy; rejection: subclinical.
© 2020 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
Disclosure
The authors of this manuscript have no conflicts to disclose as described by the
Figures




Comment in
-
Letter to the AJT Editor re: Puttarajappa et al (doi:10.1111/ajt.16150).Am J Transplant. 2021 Mar;21(3):1346-1347. doi: 10.1111/ajt.16308. Epub 2020 Oct 5. Am J Transplant. 2021. PMID: 32946671 No abstract available.
-
Author response to comments on economic analysis of subclinical rejection screening in kidney transplantation.Am J Transplant. 2021 Mar;21(3):1348-1349. doi: 10.1111/ajt.16356. Epub 2020 Oct 31. Am J Transplant. 2021. PMID: 33068499 No abstract available.
References
-
- Hoffman W, Mehta R, Jorgensen DR, et al. The Impact of Early Clinical and Subclinical T Cell-mediated Rejection After Kidney Transplantation. Transplantation. 2019;103(7):1457–1467. - PubMed
-
- Nankivell BJ, Borrows RJ, Fung CL, O’Connell PJ, Allen RD, Chapman JR. Natural history, risk factors, and impact of subclinical rejection in kidney transplantation. Transplantation. 2004;78(2):242–249. - PubMed
-
- Gloor JM, DeGoey SR, Pineda AA, et al. Overcoming a positive crossmatch in living-donor kidney transplantation. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2003;3(8):1017–1023. - PubMed
-
- Rush D, Nickerson P, Gough J, et al. Beneficial effects of treatment of early subclinical rejection: a randomized study. Journal of the American Society of Nephrology : JASN. 1998;9(11):2129–2134. - PubMed
-
- Mehta R, Sood P, Hariharan S. Subclinical Rejection in Renal Transplantation: Reappraised. Transplantation. 2016;100(8):1610–1618. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
