

The Role of Bile Acids in Chronic Diarrhea
- PMID: 32558690
- PMCID: PMC7541465
- DOI: 10.14309/ajg.0000000000000696
The Role of Bile Acids in Chronic Diarrhea
Abstract
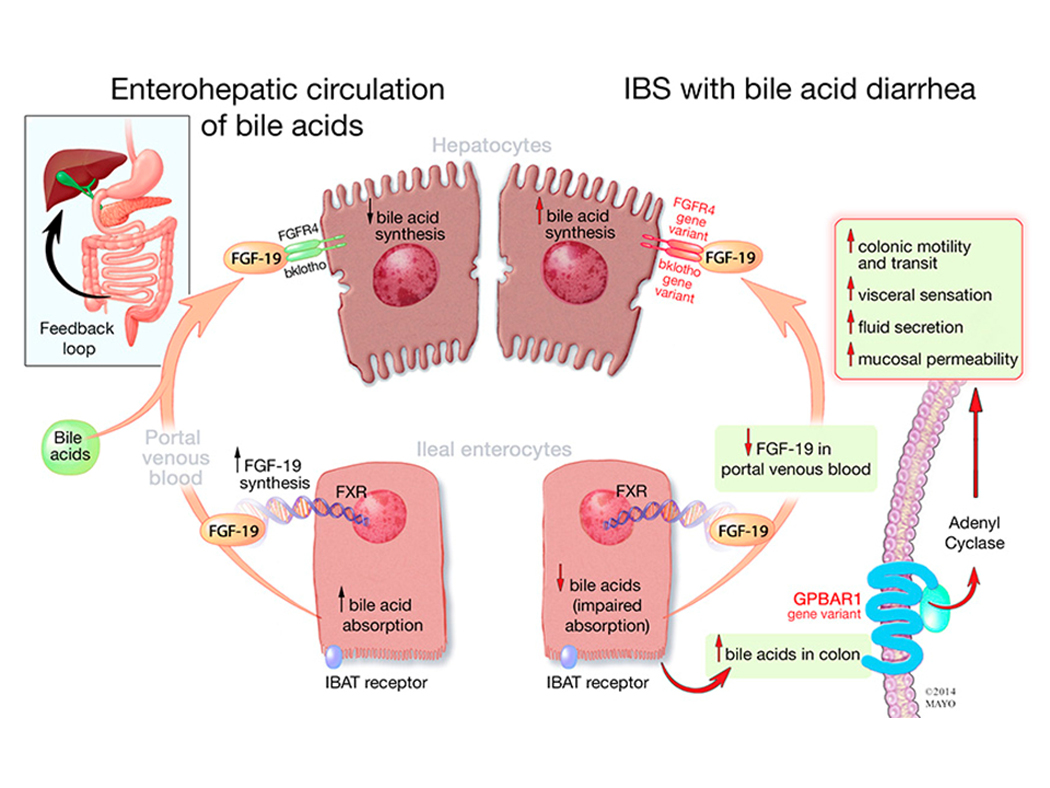
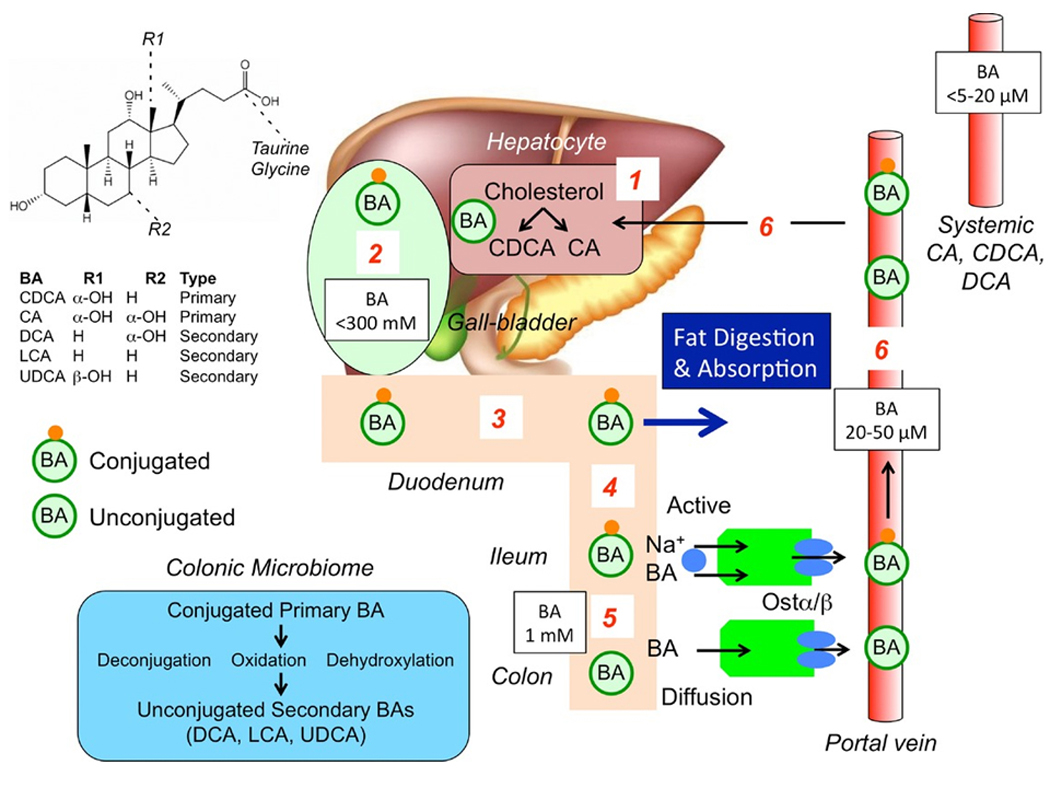
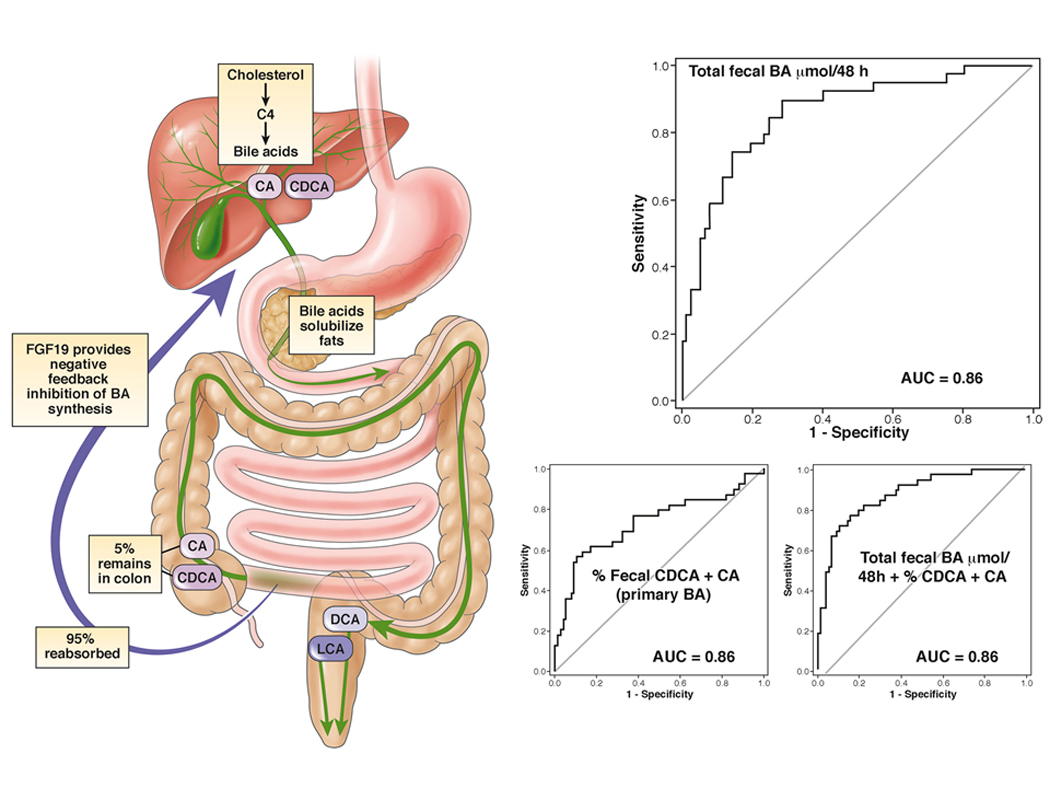
Bile acids (BAs) are the central signals in enterohepatic communication, and they also integrate microbiota-derived signals into enterohepatic signaling. The tissue distribution and signaling pathways activated by BAs through natural receptors, farsenoid X receptor and G protein-coupled BA receptor 1 (GPBAR1, also known as Takeda G-coupled receptor 5), have led to a greater understanding of the mechanisms and potential therapeutic agents. BA diarrhea is most commonly encountered in ileal resection or disease, in idiopathic disorders (with presentation similar to functional diarrhea or irritable bowel syndrome with diarrhea), and in association with malabsorption such as chronic pancreatitis or celiac disease. Diagnosis of BA diarrhea is based on Se-homocholic acid taurine retention, 48-hour fecal BA excretion, or serum 7αC4; the latter being a marker of hepatic BA synthesis. BA diarrhea tends to be associated with higher body mass index, increased stool weight and stool fat, and acceleration of colonic transit. Biochemical markers of increased BA synthesis or excretion are available through reference laboratories. Current treatment of BA diarrhea is based on BA sequestrants, and, in the future, it is anticipated that farsenoid X receptor agonists may also be effective. The optimal conditions for an empiric trial with BA sequestrants as a diagnostic test are still unclear. However, such therapeutic trials are widely used in clinical practice. Some national guidelines recommend definitive diagnosis of BA diarrhea over empirical trial.
Figures
References
-
- Wingate DL, Krag E, Mekhjian HS, et al. Relationships between ion and water movement in the human jejunum, ileum and colon during perfusion with bile acids. Clin Sci Mol Med 1973;45:593–606. - PubMed
-
- Bampton PA, Dinning PG, Kennedy ML, et al. The proximal colonic motor response to rectal mechanical and chemical stimulation. Am J Physiol Gastrointest Liver Physiol 2002;282:G443–9. - PubMed
-
- Mekhjian HS, Phillips SF, Hofmann AF. Colonic absorption of unconjugated bile acids: perfusion studies in man. Dig Dis Sci 1979;24:545–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
