

Variation in Ventilator Allocation Guidelines by US State During the Coronavirus Disease 2019 Pandemic: A Systematic Review
- PMID: 32558916
- PMCID: PMC7305526
- DOI: 10.1001/jamanetworkopen.2020.12606
Variation in Ventilator Allocation Guidelines by US State During the Coronavirus Disease 2019 Pandemic: A Systematic Review
Abstract
Importance: During the coronavirus disease 2019 pandemic, there may be too few ventilators to meet medical demands. It is unknown how many US states have ventilator allocation guidelines and how these state guidelines compare with one another.
Objective: To evaluate the number of publicly available US state guidelines for ventilator allocation and the variation in state recommendations for how ventilator allocation decisions should occur and to assess whether unique criteria exist for pediatric patients.
Evidence review: This systematic review evaluated publicly available guidelines about ventilator allocation for all states in the US and in the District of Columbia using department of health websites for each state and internet searches. Documents with any discussion of a process to triage mechanical ventilatory support during a public health emergency were screened for inclusion. Articles were excluded if they did not include specific ventilator allocation recommendations, were in draft status, did not include their state department of health, or were not the most up-to-date guideline. All documents were individually assessed and reassessed by 2 independent reviewers from March 30 to April 2 and May 8 to 10, 2020.
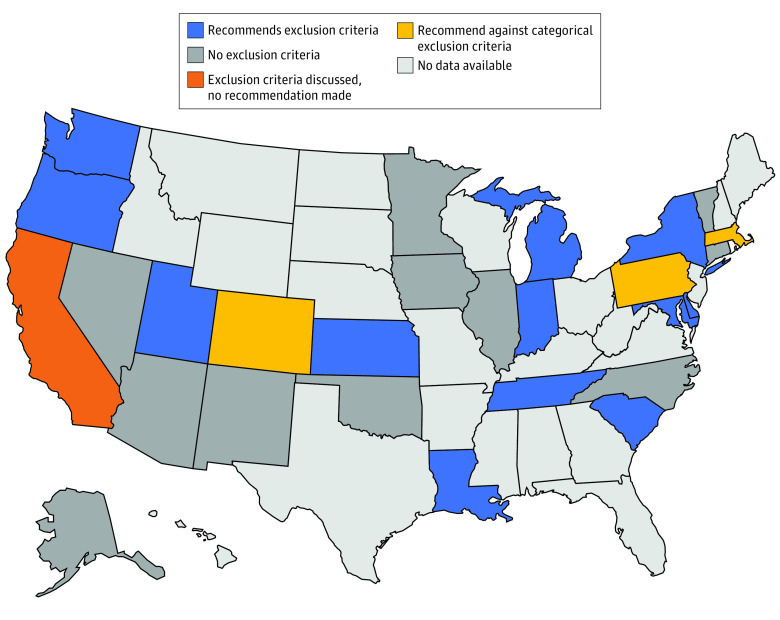
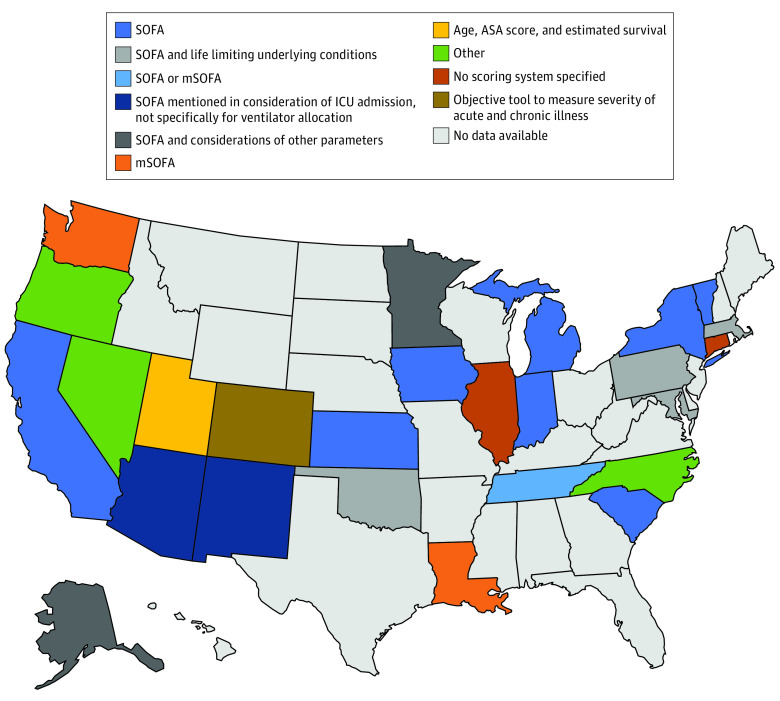
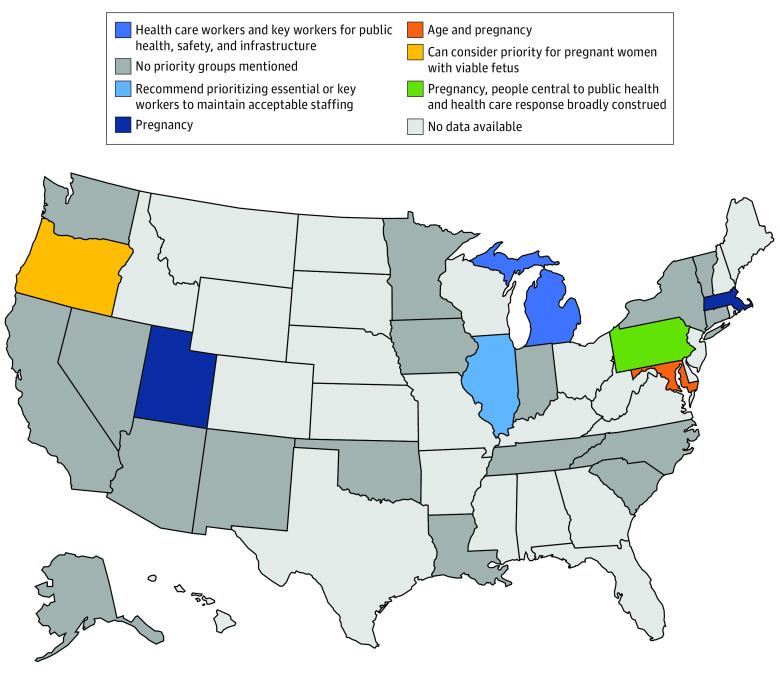
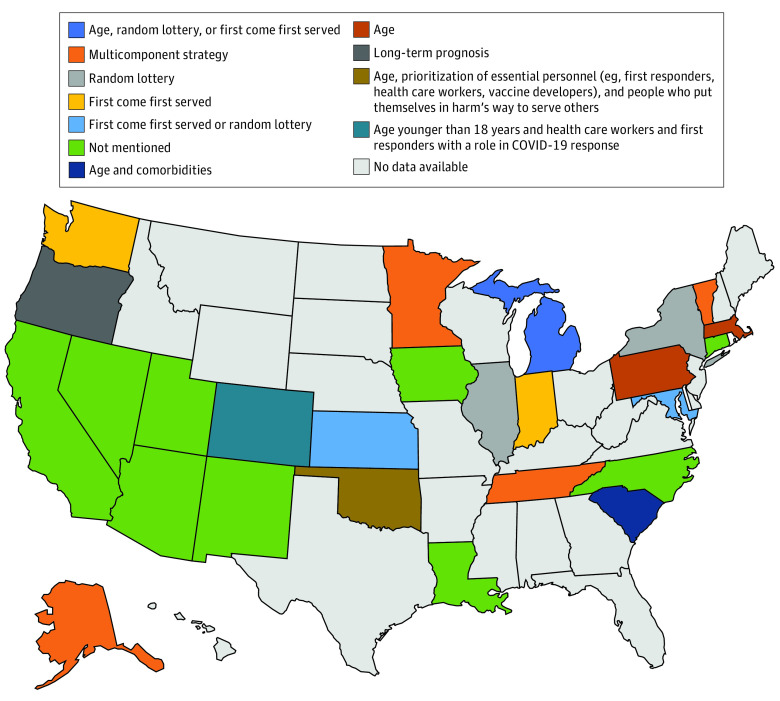
Findings: As of May 10, 2020, 26 states had publicly available ventilator guidelines, and 14 states had pediatric guidelines. Use of the Sequential Organ Failure Assessment score in the initial rank of adult patients was recommended in 15 state guidelines (58%), and assessment of limited life expectancy from underlying conditions or comorbidities was included in 6 state guidelines (23%). Priority was recommended for specific groups in the initial evaluation of patients in 6 states (23%) (ie, Illinois, Maryland, Massachusetts, Michigan, Pennsylvania, and Utah). Many states recommended exclusion criteria in adult (11 of 26 states [42%]) and pediatric (10 of 14 states [71%]) ventilator allocation. Withdrawal of mechanical ventilation from a patient to give to another if a shortage occurs was discussed in 22 of 26 adult guidelines (85%) and 9 of 14 pediatric guidelines (64%).
Conclusions and relevance: These findings suggest that although allocation guidelines for mechanical ventilatory support are essential in a public health emergency, only 26 US states provided public guidance on how this allocation should occur. Guidelines among states, including adjacent states, varied significantly and could cause inequity in the allocation of mechanical ventilatory support during a public health emergency, such as the coronavirus disease 2019 pandemic.
Conflict of interest statement
Figures
Comment in
-
Improving Ventilator Rationing Through Collaboration With Experts on Resource Allocation.JAMA Netw Open. 2020 Jun 1;3(6):e2012838. doi: 10.1001/jamanetworkopen.2020.12838. JAMA Netw Open. 2020. PMID: 32558911 No abstract available.
References
-
- Calabresi G. Tragic Choices. W. W. Norton & Co; 1978.
-
- Christian MD, Devereaux AV, Dichter JR, Rubinson L, Kissoon N; Task Force for Mass Critical Care; Task Force for Mass Critical Care . Introduction and executive summary: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014;146(4)(suppl):8S-34S. doi:10.1378/chest.14-0732 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
