Acute and chronic sympathomimetic effects of e-cigarette and tobacco cigarette smoking: role of nicotine and non-nicotine constituents
- PMID: 32559135
- PMCID: PMC7473924
- DOI: 10.1152/ajpheart.00192.2020
Acute and chronic sympathomimetic effects of e-cigarette and tobacco cigarette smoking: role of nicotine and non-nicotine constituents
Abstract
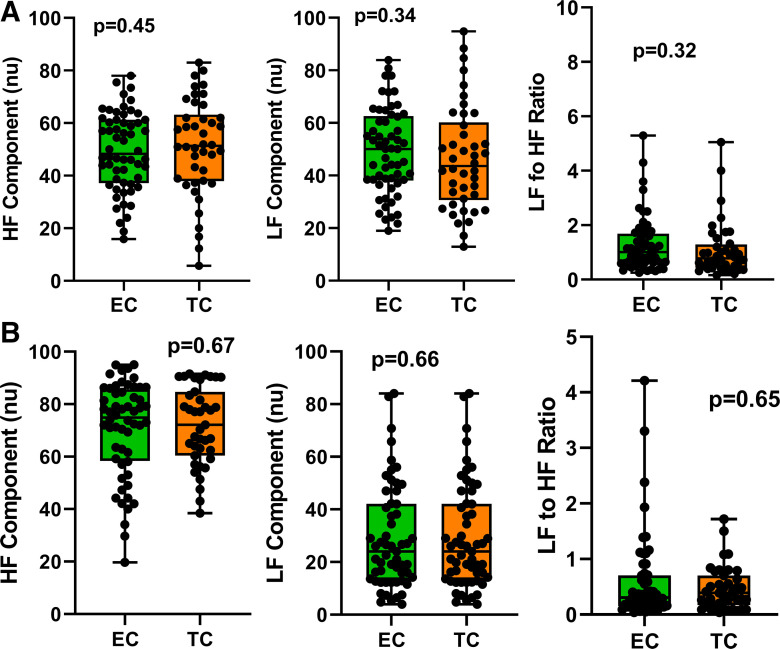
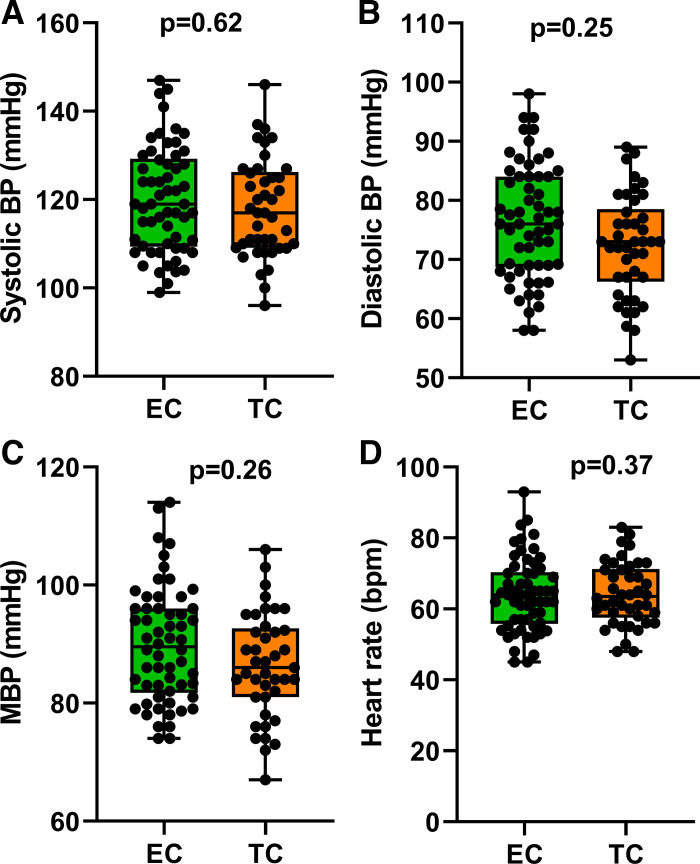
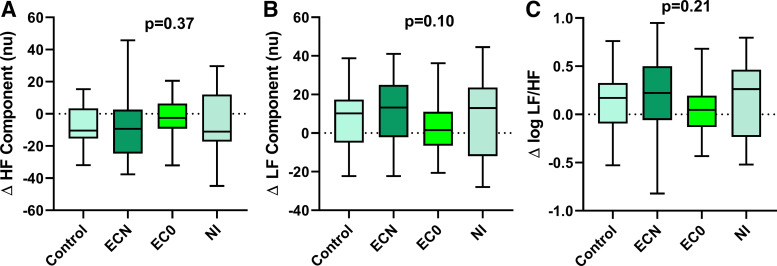
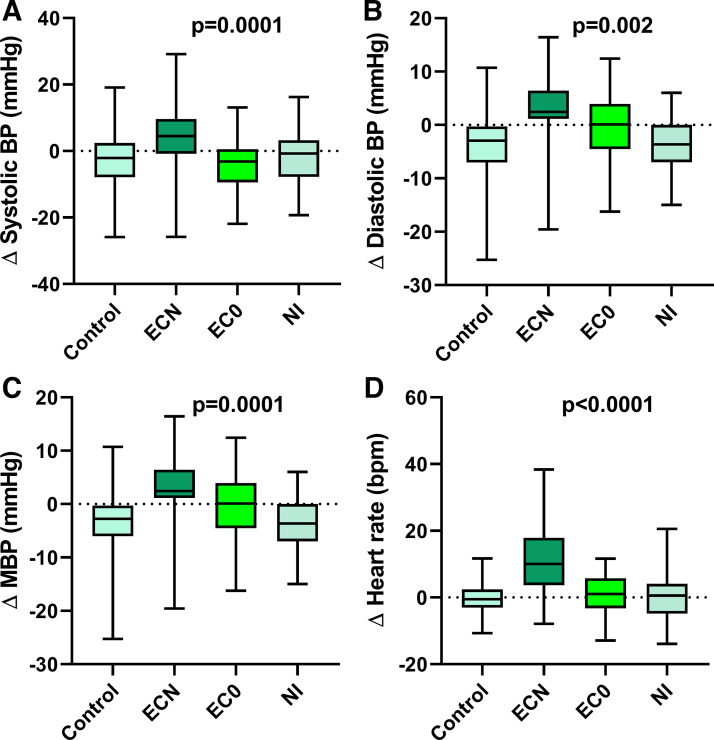
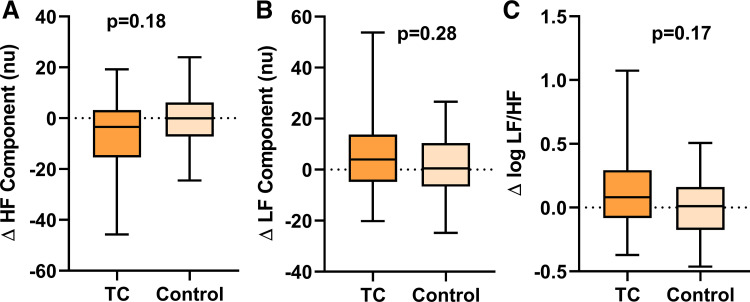
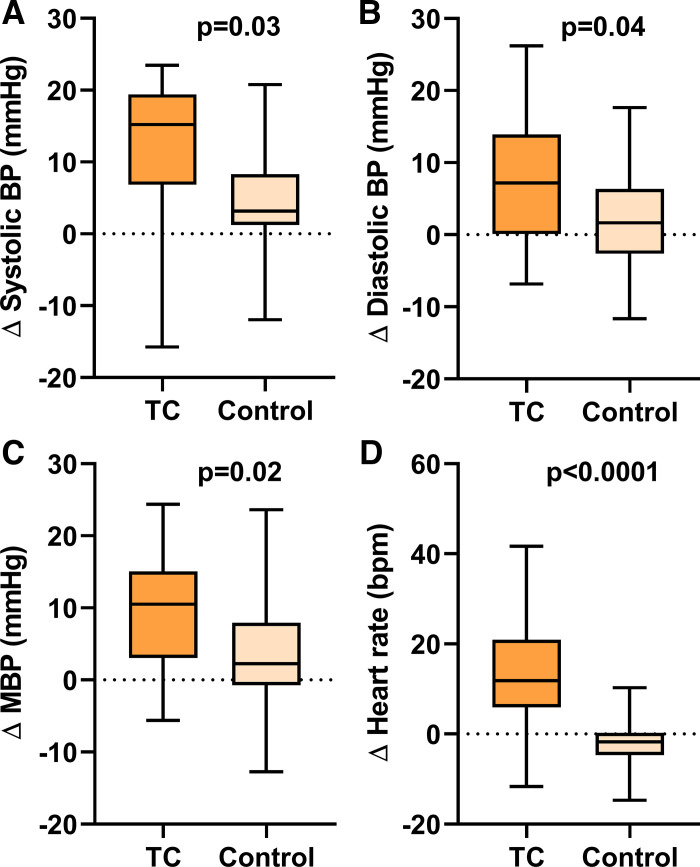
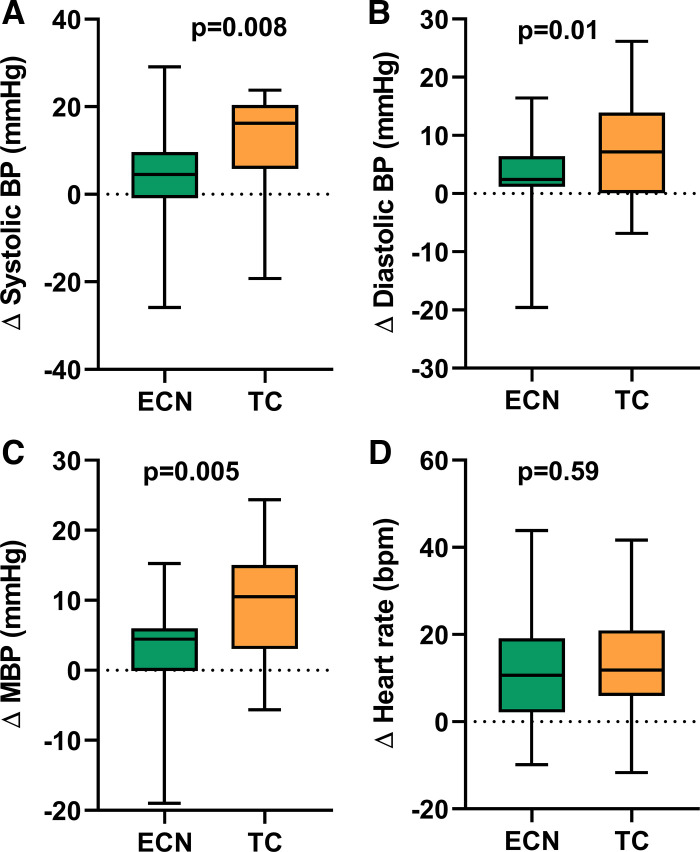
Electronic cigarettes (ECs) and tobacco cigarettes (TCs) both release nicotine, a sympathomimetic drug. We hypothesized that baseline heart rate variability (HRV) and hemodynamics would be similar in chronic EC and TC smokers and that after acute EC use, changes in HRV and hemodynamics would be attributable to nicotine, not non-nicotine, constituents in EC aerosol. In 100 smokers, including 58 chronic EC users and 42 TC smokers, baseline HRV and hemodynamics [blood pressure (BP) and heart rate (HR)] were compared. To isolate the acute effects of nicotine vs. non-nicotine constituents in EC aerosol, we compared changes in HRV, BP, and HR in EC users after using an EC with nicotine (ECN), EC without nicotine (EC0), nicotine inhaler (NI), or sham vaping (control). Outcomes were also compared with TC smokers after smoking one TC. Baseline HRV and hemodynamics were not different in chronic EC users and TC smokers. In EC users, BP and HR, but not HRV outcomes, increased only after using the ECN, consistent with a nicotine effect on BP and HR. Similarly, in TC smokers, BP and HR but not HRV outcomes increased after smoking one TC. Despite a similar increase in nicotine, the hemodynamic increases were significantly greater after TC smokers smoked one TC compared with the increases after EC users used the ECN. In conclusion, chronic EC and TC smokers exhibit a similar pattern of baseline HRV. Acute increases in BP and HR in EC users are attributable to nicotine, not non-nicotine, constituents in EC aerosol. The greater acute pressor effects after TC compared with ECN may be attributable to non-nicotine, combusted constituents in TC smoke.NEW & NOTEWORTHY Chronic electronic cigarette (EC) users and tobacco cigarette (TC) smokers exhibit a similar level of sympathetic nerve activity as estimated by heart rate variability. Acute increases in blood pressure (BP) and heart rate in EC users are attribute to nicotine, not non-nicotine, constituents in EC aerosol. Acute TC smoking increased BP significantly more than acute EC use, despite similar increases in plasma nicotine, suggestive of additional adverse vascular effects attributable to combusted, non-nicotine constituents in TC smoke.
Keywords: blood pressure; electronic cigarettes; heart rate variability; nicotine; tobacco cigarettes.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures