

COVID-19 Diagnostics, Tools, and Prevention
- PMID: 32560091
- PMCID: PMC7344926
- DOI: 10.3390/diagnostics10060409
COVID-19 Diagnostics, Tools, and Prevention
Abstract
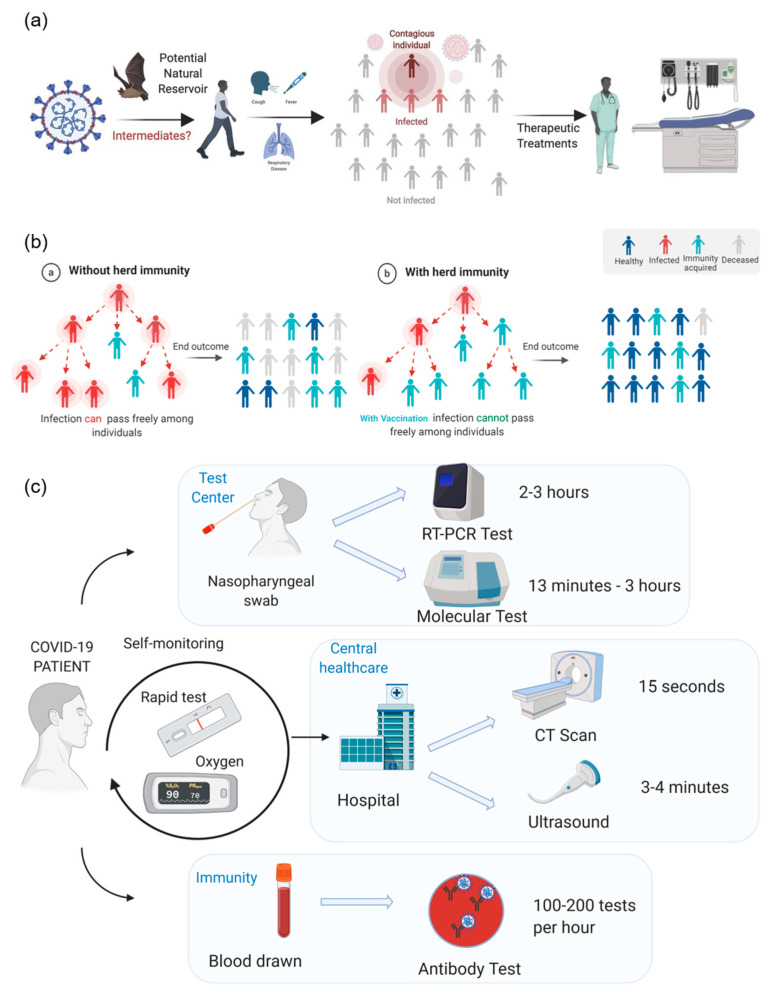
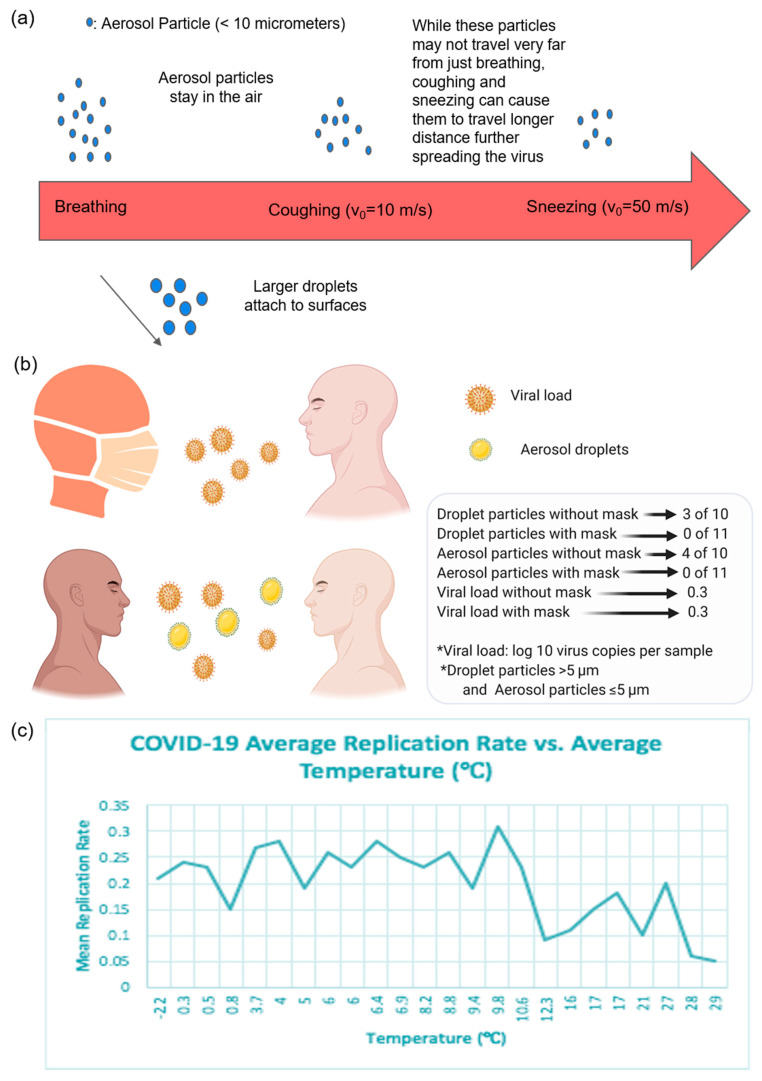
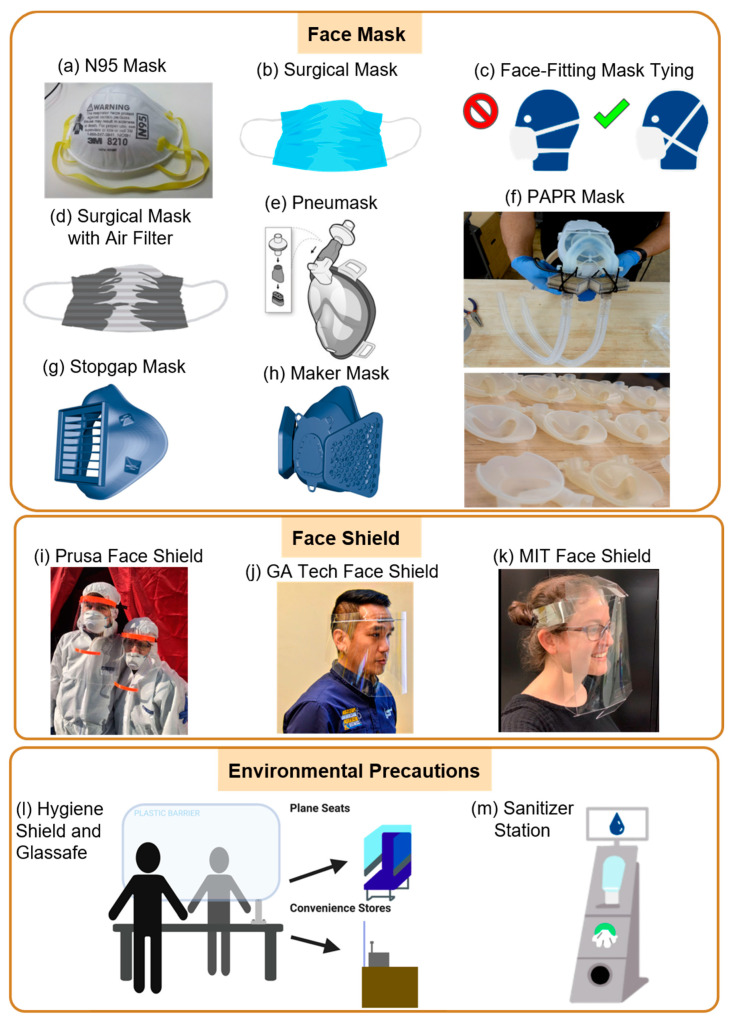
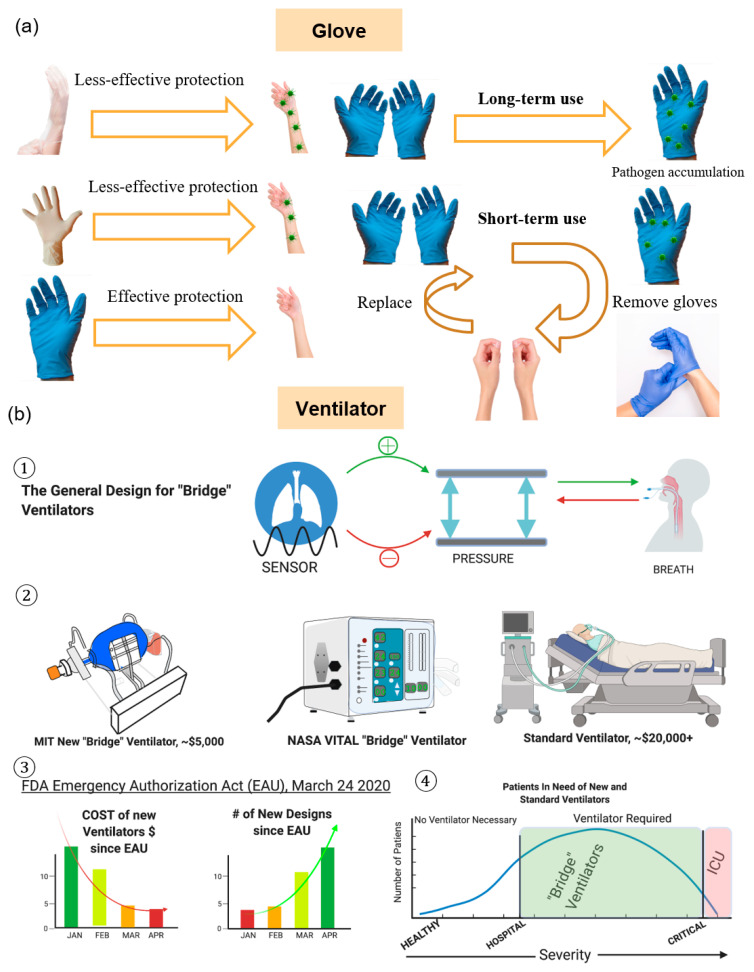
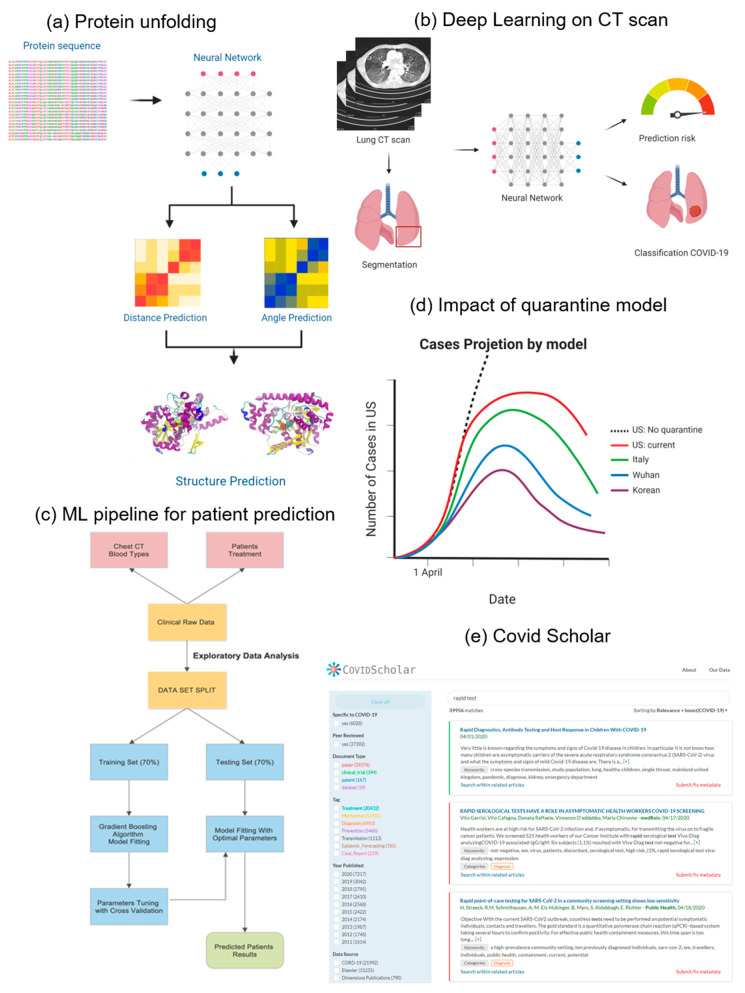
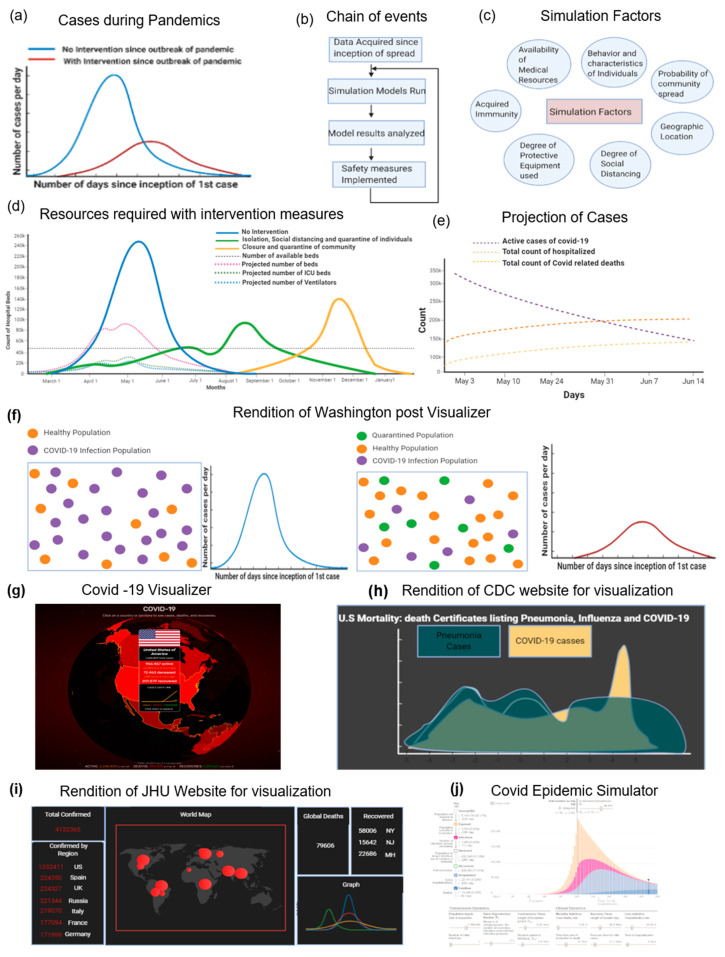
The Coronavirus Disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), outbreak from Wuhan City, Hubei province, China in 2019 has become an ongoing global health emergency. The emerging virus, SARS-CoV-2, causes coughing, fever, muscle ache, and shortness of breath or dyspnea in symptomatic patients. The pathogenic particles that are generated by coughing and sneezing remain suspended in the air or attach to a surface to facilitate transmission in an aerosol form. This review focuses on the recent trends in pandemic biology, diagnostics methods, prevention tools, and policies for COVID-19 management. To meet the growing demand for medical supplies during the COVID-19 era, a variety of personal protective equipment (PPE) and ventilators have been developed using do-it-yourself (DIY) manufacturing. COVID-19 diagnosis and the prediction of virus transmission are analyzed by machine learning algorithms, simulations, and digital monitoring. Until the discovery of a clinically approved vaccine for COVID-19, pandemics remain a public concern. Therefore, technological developments, biomedical research, and policy development are needed to decipher the coronavirus mechanism and epidemiological characteristics, prevent transmission, and develop therapeutic drugs.
Keywords: 3D printing; COVID-19; SARS-CoV-2; digital tracking; do-it-yourself; immunity; machine learning; pandemic policy; rapid testing; vaccines.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Cascella M., Rajnik M., Cuomo A., Dulebohn S.C., Di Napoli R. StatPearls. StatPearls Publishing; Treasure Island, FL, USA: 2020. Features, Evaluation and Treatment Coronavirus (COVID-19) - PubMed
-
- Madhav N., Oppenheim B., Gallivan M., Mulembakani P., Rubin E., Wolfe N. Pandemics: Risks, Impacts, and Mitigation. In: Jamison D.T., Gelband H., Horton S., Jha P., Laxminarayan R., Mock C.N., Nugent R., editors. Disease Control Priorities: Improving Health and Reducing Poverty. The International Bank for Reconstruction and Development/The World Bank; Washington, DC, USA: 2017. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
