

The epidemiology of carbapenem-non-susceptible Acinetobacter species in Europe: analysis of EARS-Net data from 2013 to 2017
- PMID: 32560670
- PMCID: PMC7304165
- DOI: 10.1186/s13756-020-00750-5
The epidemiology of carbapenem-non-susceptible Acinetobacter species in Europe: analysis of EARS-Net data from 2013 to 2017
Abstract
Background: Due to limited therapeutic options and their association with high mortality and morbidity, carbapenem-non-susceptible Acinetobacter spp. (CNA) are of significant public health importance. This study aimed to describe current epidemiological trends of CNA proportions in Europe and to identify factors that are associated with carbapenem non-susceptibility of isolates from patients with invasive Acinetobacter spp. infections.
Methods: Data from routine carbapenem susceptibility testing of 18,412 invasive clinical Acinetobacter spp. isolates from 30 European countries in 2013-2017 were analysed using descriptive statistical analyses and uni- and multivariable regression analyses. These data were obtained from the European Antimicrobial Resistance Surveillance Network (EARS-Net).
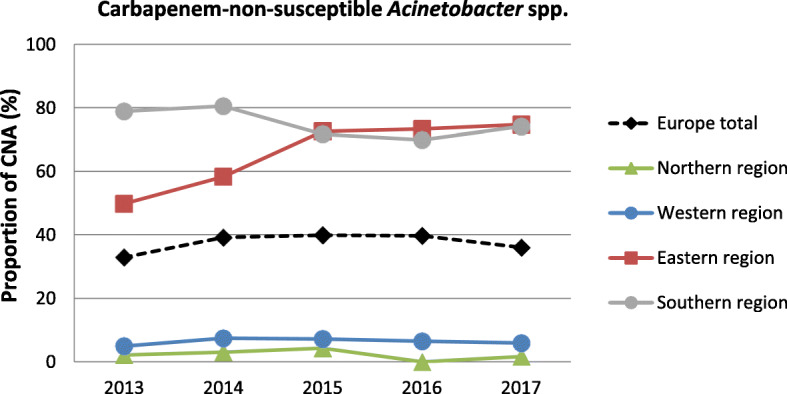
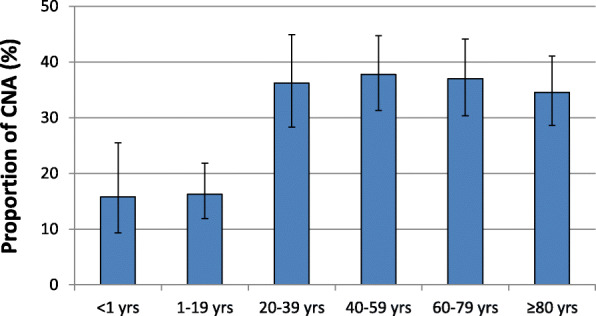
Results: The population-weighted mean proportion of carbapenem-non-susceptible Acinetobacter spp. in Europe is 35.6% (95% confidence interval [CI] 29.7-42.0%). With CNA proportions of 75.5% (95% CI 71.2-79.4%) and 71.5% (95% CI 66.7-75.9%) the burden of CNA is particularly high in Southern and Eastern European regions. In contrast, Northern and Western European regions recorded CNA proportions of 2.8% (95% CI 1.2-6.0%) and 6.3% (95% CI 4.5-8.9%), respectively. Population-weighted mean CNA proportions are especially high in Acinetobacter spp. isolates from intensive care units (54.0% [95% CI 47.6-60.3%]). Male gender, age above 20 years and ICU admission were identified as independent factors associated with an increased likelihood of CNA.
Conclusion: The burden of carbapenem-non-susceptible Acinetobacter spp. is particularly high in Southern and Eastern Europe. There is a risk that resistance could spread to other parts of Europe. Therefore, increased efforts in infection control and antibiotic stewardship, particularly in Intensive Care Units, are necessary to combat the spread of CNA in Europe.
Keywords: Acinetobacter; Acinetobacter baumannii; Antimicrobial resistance; Carbapenem resistance; EARS-Net; Surveillance.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- ECDC . Carbapenem-resistant Acinetobacter baumanni in healthcare settings. Stockholm: European Centre for Disease Prevention and Control; 2016.
-
- Fournier PE, Richet H. The epidemiology and control of Acinetobacter baumannii in health care facilities. Clin Infect Dis. 2006;42(5):692–699. - PubMed
-
- Karah N, et al. Insights into the global molecular epidemiology of carbapenem non-susceptible clones of Acinetobacter baumannii. Drug Resist Updat. 2012;15(4):237–247. - PubMed
-
- Munoz-Price LS, Weinstein RA. Acinetobacter infection. N Engl J Med. 2008;358(12):1271–1281. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
