

Population-Based Assessment of Aortic-Related Outcomes in Aortic Dissection, Intramural Hematoma, and Penetrating Aortic Ulcer
- PMID: 32561245
- PMCID: PMC9680920
- DOI: 10.1016/j.avsg.2020.06.004
Population-Based Assessment of Aortic-Related Outcomes in Aortic Dissection, Intramural Hematoma, and Penetrating Aortic Ulcer
Abstract
Background: The aim of the study was to analyze aortic-related outcomes after diagnosis of aortic dissection (AD), intramural hematoma (IMH), and penetrating aortic ulcer (PAU) from a population-based approach.
Methods: Retrospective review of an incident cohort of AD, IMH, and PAU patients in Olmsted County, Minnesota from 1995 to 2015. Primary end point was aortic death. Secondary end points were subsequent aortic events (aortic intervention, new dissection, or rupture not present at presentation) and first-time diagnosis of an aortic aneurysm. Outcomes were compared with randomly selected population referents matched for age and sex in a 3:1 ratio using Cox proportional hazards regression adjusting for comorbidities.
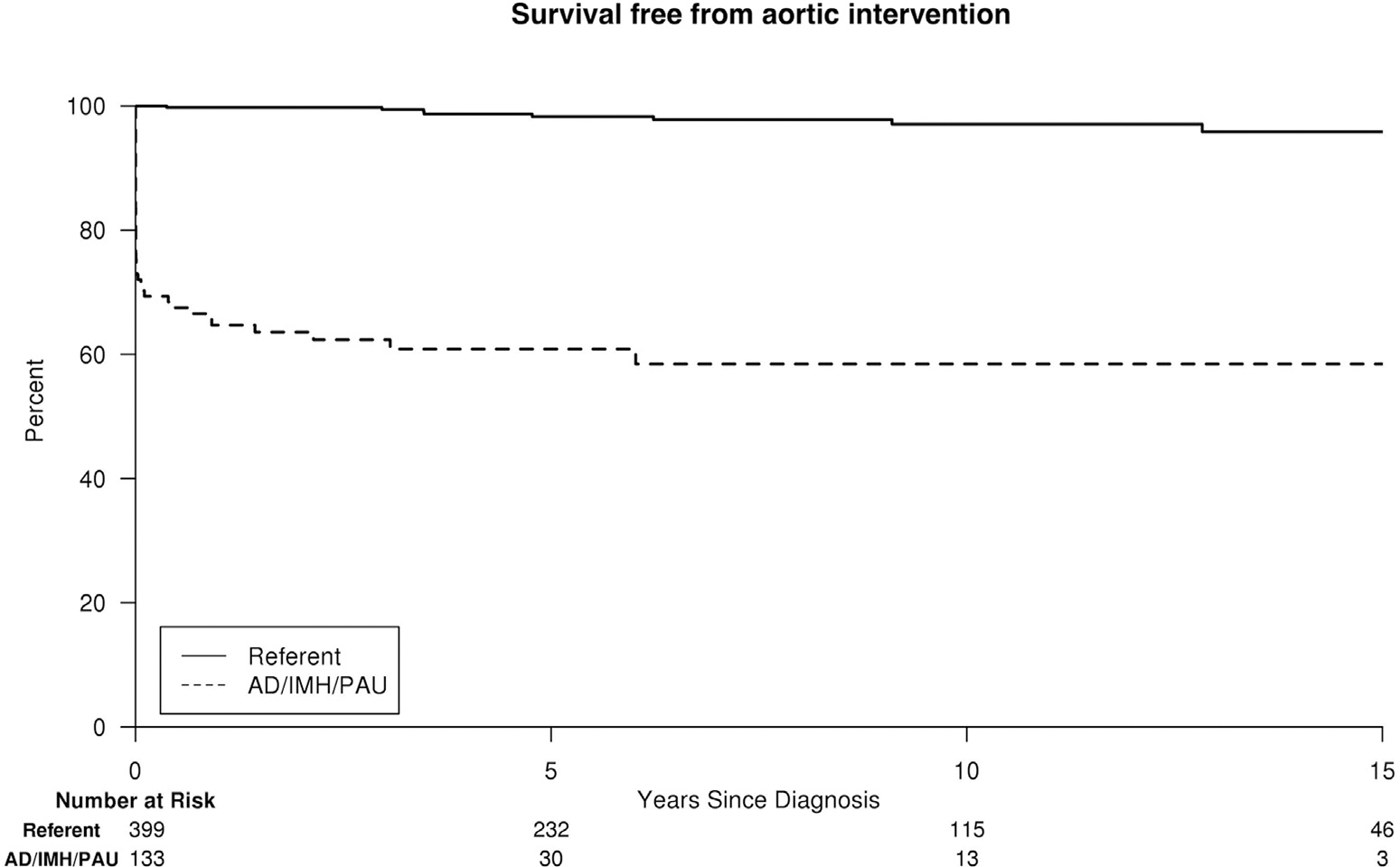
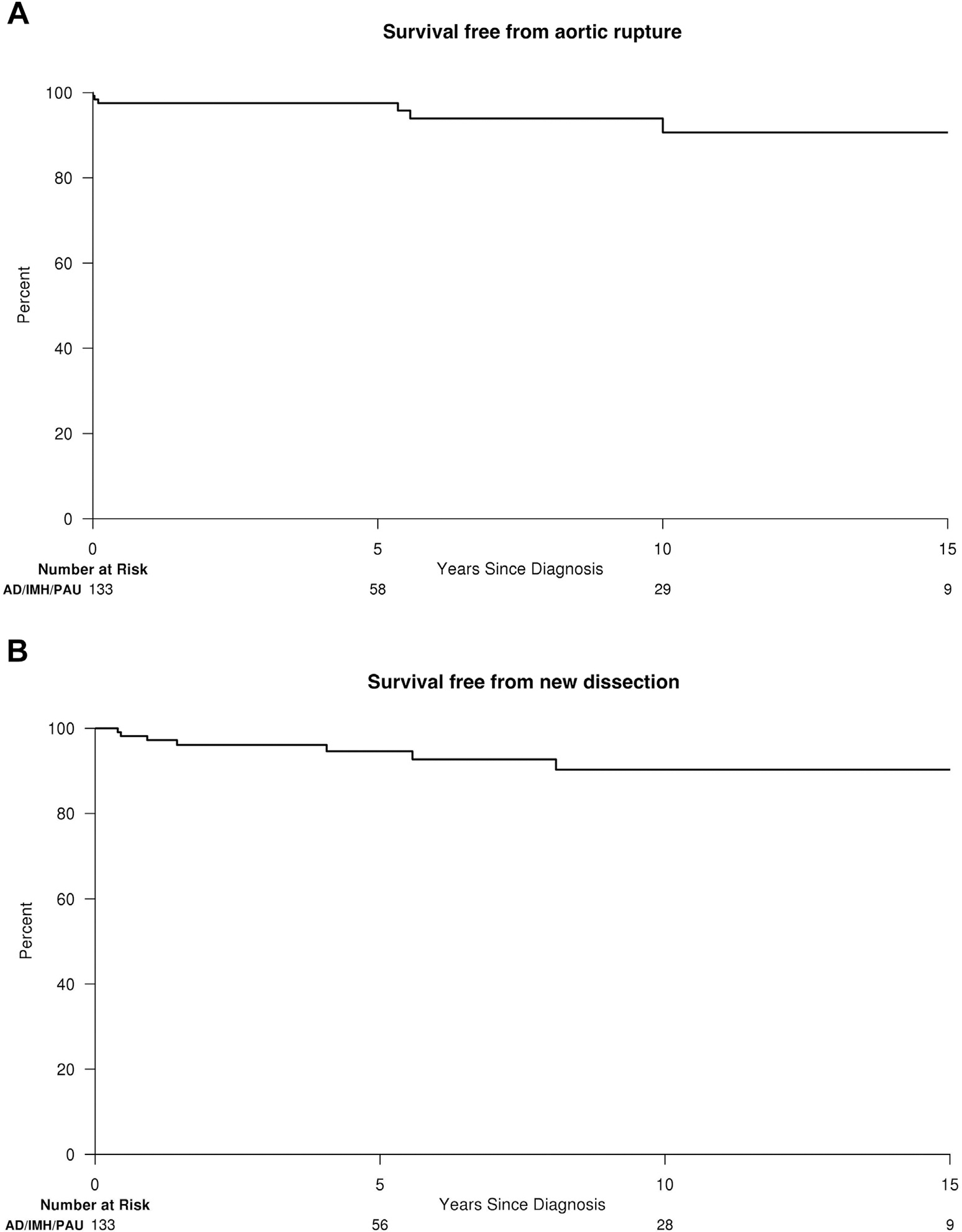
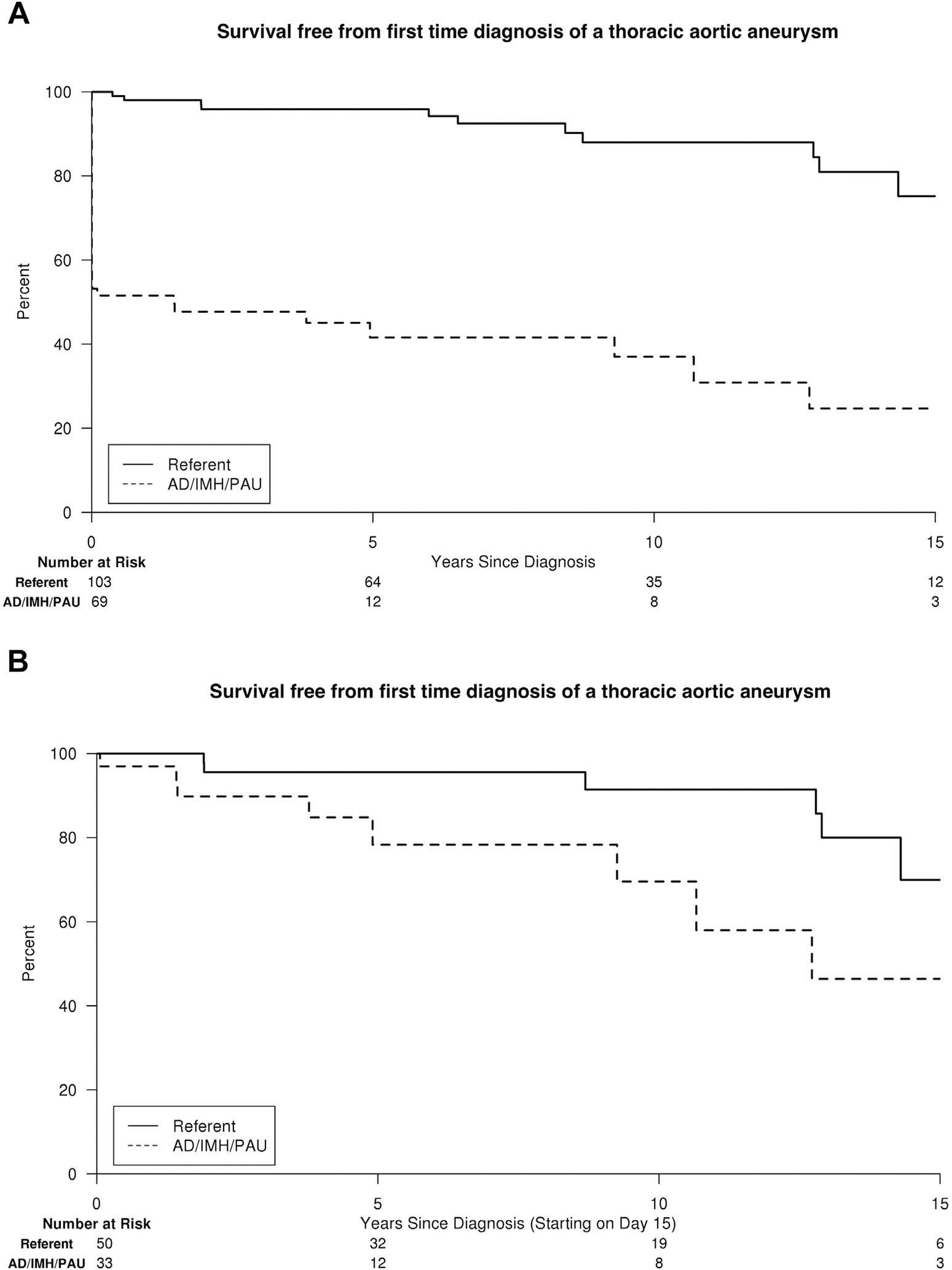
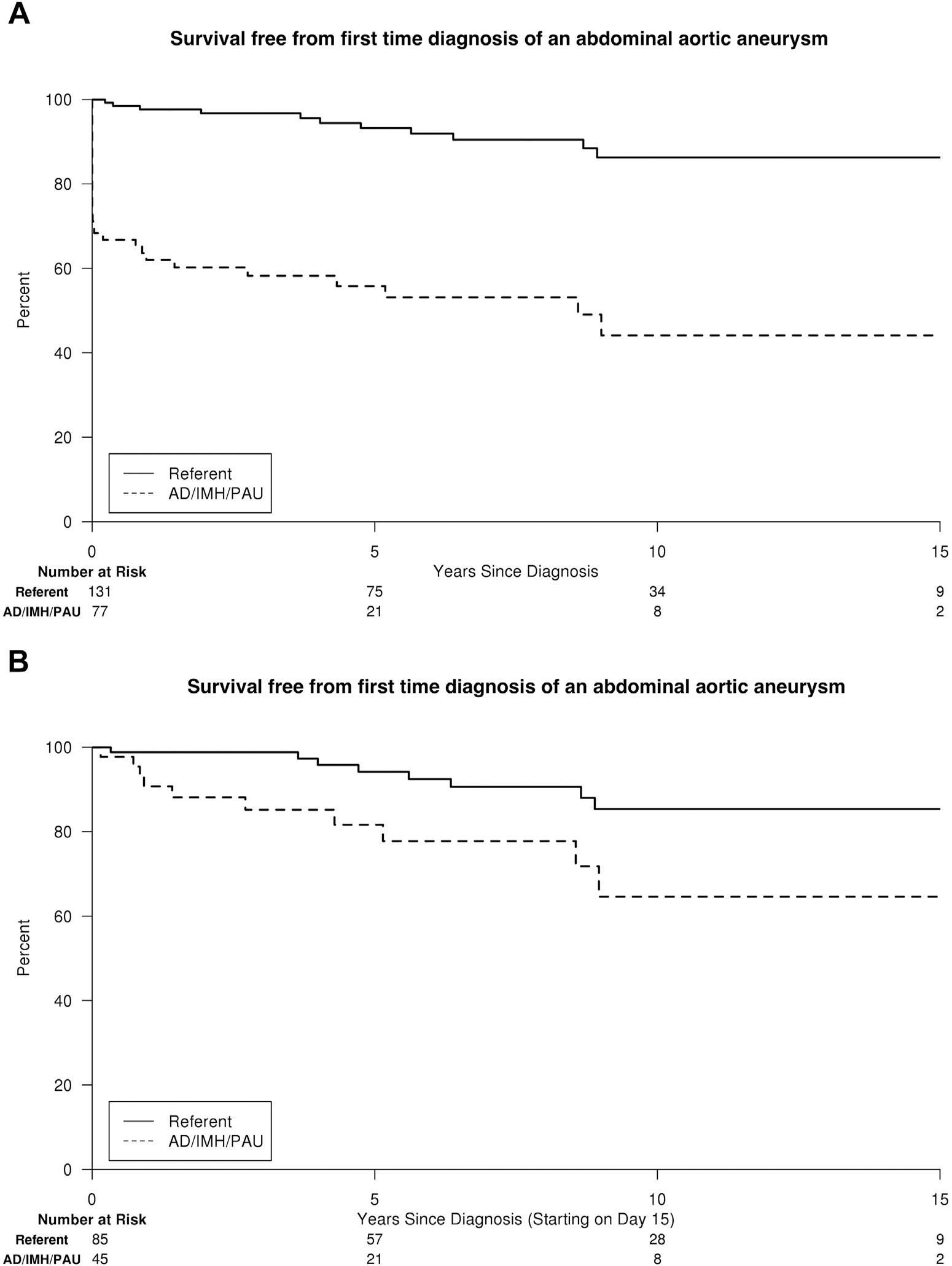
Results: Among 133 patients (77 AD, 21 IMH, and 35 PAU), 57% were males, and mean age was 71.8 years (standard deviation, 14). Median follow-up was 10 years. Of 73 deaths among AD/IMH/PAU patients, 23 (32%) were aortic-related. Estimated freedom from aortic death was 84%, 80%, and 77% at 5, 10, and 15 years. There were no aortic deaths among population referents (adjusted hazard ratio [HR] for aortic death in AD/IMH/PAU, 184.7; 95% confidence interval [95% CI], 10.3-3,299.2; P < 0.001). Fifty (38%) AD/IMH/PAU patients had a subsequent aortic event (aortic intervention, new dissection, or rupture), whereas there were 8 (2%) aortic events among population referents (all elective aneurysm repairs; adjusted HR for any aortic event and aortic intervention in AD/IMH/PAU patients, 33.3; 95% CI, 15.3-72.0; P < 0.001 and 31.5; 95% CI, 14.5-68.4; P < 0.001, respectively). After excluding aortic events/interventions ≤14 days of diagnosis, AD/IMH/PAU patients remained at increased risk of any aortic event (adjusted HR, 10.8; 95% CI, 3.9-29.8; P < 0.001) and aortic intervention (adjusted HR, 9.6; 95% CI, 3.4-26.8; P < 0.001). Among those subjects with available follow-up imaging, the risk of first-time diagnosis of aortic aneurysm was significantly increased for AD/IMH/PAU patients when compared with population referents (adjusted HR, 10.9; 95% CI, 5.4-21.7; P < 0.001 and 8.3; 95% CI, 4.1-16.7; P < 0.001 for thoracic and abdominal aneurysms, respectively) and remained increased when excluding aneurysms that formed within 14 days of AD/IMH/PAU (adjusted HR, 6.2; 95% CI, 1.8-21.1; P = 0.004 and 2.8; 95% CI, 1.0-7.6; P = 0.040 for thoracic and abdominal aneurysms, respectively).
Conclusions: AD/IMH/PAU patients have a substantial risk of aortic death, any aortic event, aortic intervention, and first-time diagnosis of aortic aneurysm that persists even when the acute phase (≤14 days after diagnosis) is uncomplicated. Advances in postdiagnosis treatment are necessary to improve the prognosis in these patients.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Riambau V, Bockler D, J Brunkwall, et al. Editor’s choice—management of descending thoracic aorta diseases: clinical practice guidelines of the European Society for Vascular surgery (ESVS). Eur J Vasc Endovasc Surg 2017;53:4–52. - PubMed
-
- Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation 2005;112:3802–13. - PubMed
-
- Pape LA, Awais M, Woznicki EM, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection. J Am Coll Cardiol 2015;66:350–8. - PubMed
-
- Tsai TT, Fattori R, Trimarchi S, et al. Long-term survival in patients presenting with type B acute aortic dissection: insights from the International Registry of Acute Aortic Dissection. Circulation 2006;114:2226–31. - PubMed
-
- Umana JP, Lai DT, Mitchell RS, et al. Is medical therapy still the optimal treatment strategy for patients with acute type B aortic dissections? J Thorac Cardiovasc Surg 2002;124: 896–910. - PubMed
