

Subtypes of dementia with Lewy bodies are associated with α-synuclein and tau distribution
- PMID: 32561678
- PMCID: PMC7455327
- DOI: 10.1212/WNL.0000000000009763
Subtypes of dementia with Lewy bodies are associated with α-synuclein and tau distribution
Abstract
Objective: To determine whether Lewy body disease subgroups have different clinical profiles.
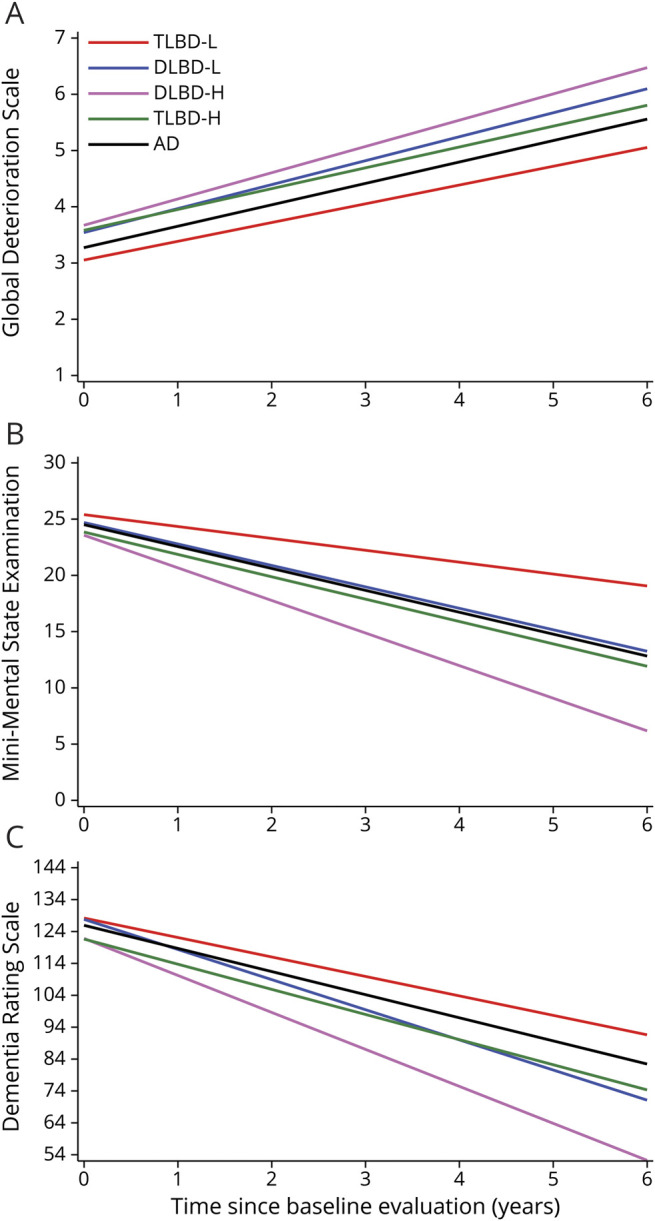
Methods: Participants had dementia, autopsy-confirmed transitional or diffuse Lewy body disease (TLBD or DLBD) (n = 244), or Alzheimer disease (AD) (n = 210), and were seen at least twice (mean follow-up 6.2 ± 3.8 years). TLBD and DLBD groups were partitioned based on the presence or absence of neocortical neurofibrillary tangles using Braak staging. Four Lewy body disease subgroups and AD were compared on clinical features, dementia trajectory, and onset latency of probable dementia with Lewy bodies (DLB) or a DLB syndrome defined as probable DLB or dementia with one core feature of parkinsonism or probable REM sleep behavior disorder.
Results: In TLBD and DLBD without neocortical tangles, diagnostic sensitivity was strong for probable DLB (87% TLBD, 96% DLBD) and the DLB syndrome (97% TLBD, 98% DLBD) with median latencies <1 year from cognitive onset, and worse baseline attention-visual processing but better memory-naming scores than AD. In DLBD with neocortical tangles, diagnostic sensitivity was 70% for probable DLB and 77% for the DLB syndrome with respective median latencies of 3.7 years and 2.7 years from cognitive onset, each associated with tangle distribution. This group had worse baseline attention-visual processing than AD, but comparable memory-naming impairment. TLBD with neocortical tangles had 48% diagnostic sensitivity for probable DLB and 52% for the DLB syndrome, with median latencies >6 years from cognitive onset, and were cognitively similar to AD. Dementia trajectory was slowest for TLBD without neocortical tangles, and fastest for DLBD with neocortical tangles.
Conclusions: The phenotypic expression of DLB was associated with the distribution of α-synuclein and tau pathology.
© 2020 American Academy of Neurology.
Figures


References
-
- Barker WW, Luis CA, Kashuba A, et al. . Relative frequencies of Alzheimer disease, Lewy body, vascular and frontotemporal dementia, and hippocampal sclerosis in the State of Florida Brain Bank. Alzheimer Dis Assoc Disord 2002;16:203–212. - PubMed
-
- Merdes AR, Hansen LA, Jeste DV, et al. . Influence of Alzheimer pathology on clinical diagnostic accuracy in dementia with Lewy bodies. Neurology 2003;60:1586–1590. - PubMed
-
- Del Ser T, Hachinski V, Merskey H, Munoz DG. Clinical and pathologic features of two groups of patients with dementia with Lewy bodies: effect of coexisting Alzheimer-type lesion load. Alzheimer Dis Assoc Disord 2001;15:31–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous