

Invasive solid papillary carcinoma with neuroendocrine differentiation of the breast: a case report and literature review
- PMID: 32562013
- PMCID: PMC7305294
- DOI: 10.1186/s40792-020-00905-x
Invasive solid papillary carcinoma with neuroendocrine differentiation of the breast: a case report and literature review
Abstract
Background: Solid papillary carcinoma (SPC) of the breast is a rare breast cancer that accounts for less than 1% of all breast cancers. The optimal clinical management of SPC remains controversial. Here, we report a case of invasive SPC with neuroendocrine differentiation in addition to review of the current literature.
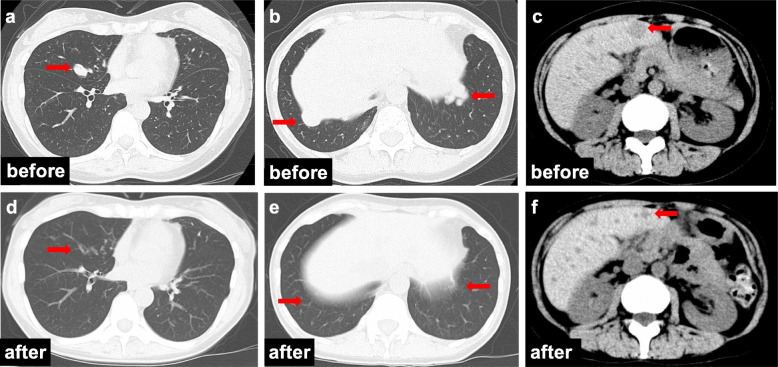
Case presentation: A premenopausal 46-year-old female presented with a mass in her left breast that tended to increase in size over a 10-month period. Mammography and ultrasonography revealed a mass in the left upper-inner quadrant. The resulting images suggested a category 3 breast tumor according to the Breast Imaging Reporting and Data System (BI-RADS). A core needle biopsy (CNB) was performed, and the pathological findings showed a solid papillary pattern and atypical cells suggestive of noninvasive SPC. After a left partial mastectomy and sentinel lymph node biopsy (SLNB), the specimens were sent for histopathological analysis for further investigation. Postoperative pathological findings suggested invasive SPC. Whole-breast radiation therapy and adjuvant hormonal therapy were performed as postoperative treatments. Three years after surgery, multiple lung metastases were detected, and the patient was treated with a gonadotropin-releasing hormone agonist and an aromatase inhibitor. Five months later, multiple liver metastases and bone metastases appeared, and oral 5-fluorouracil was chosen for the subsequent treatment. The patient has been treated for 5 years to date, and she is continuing to take oral 5-fluorouracil and is alive without any further disease progression.
Conclusions: We report a rare case of premenopausal invasive SPC with multiple metastases. Further study is needed to clarify the molecular characteristics and clinical behaviors of SPC and to explore the optimal treatment strategy.
Keywords: Breast; Invasive solid papillary carcinoma; Metastasis; Neuroendocrine differentiation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
LinkOut - more resources
Full Text Sources
