

ART strategies in Klinefelter syndrome
- PMID: 32562095
- PMCID: PMC7492331
- DOI: 10.1007/s10815-020-01818-2
ART strategies in Klinefelter syndrome
Abstract
Purpose: Patients with Klinefelter syndrome (KS) who receive assisted reproductive technology (ART) treatment often experience poor pregnancy rates due to decreased fertilization, cleavage, and implantation rates and even an increased miscarriage rate. Mounting evidence from recent studies has shown that various technological advances and approaches could facilitate the success of ART treatment for KS patients. In this review, we summarize the methods for guiding KS patients during ART and for developing optimal strategies for preserving fertility, improving pregnancy rate and live birth rate, and avoiding the birth of KS infants.
Methods: We searched PubMed and Google Scholar publications related to KS patients on topics of controlled ovarian stimulation protocols, sperm extraction, fertility preservation, gamete artificial activation, round spermatid injection (ROSI), and non-invasive prenatal screening (PGD) methods.
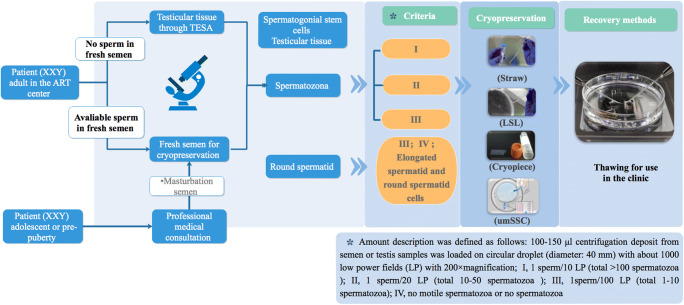
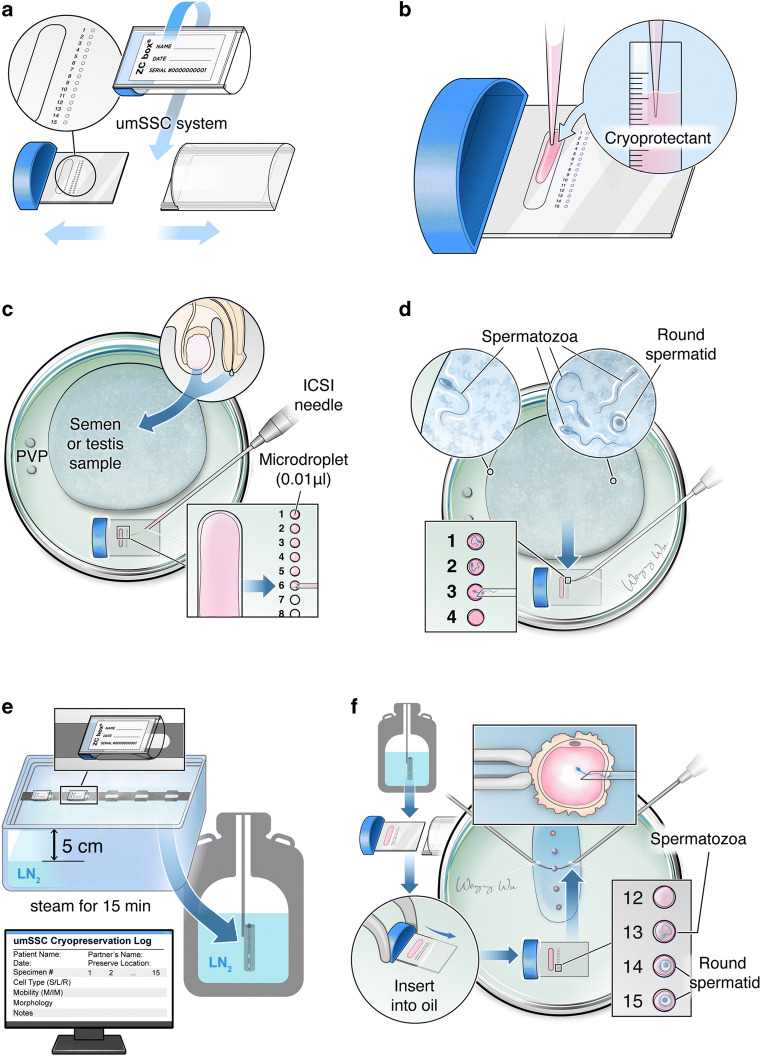
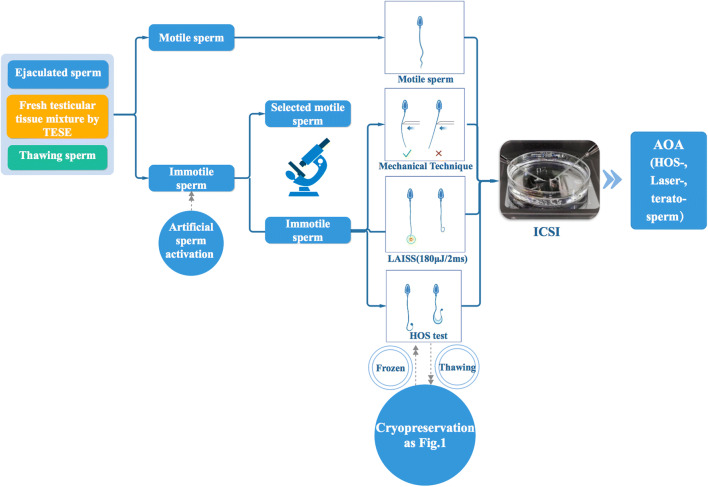
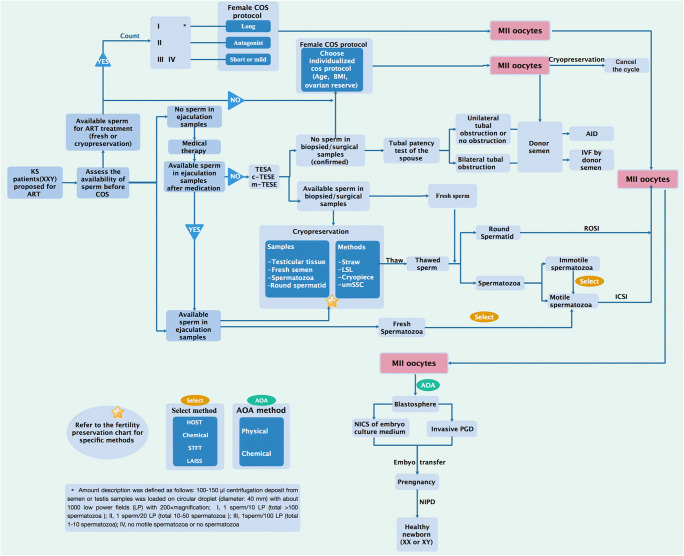
Results: This review outlines the different ovulation-inducing treatments for female partners according to the individual sperm status in the KS patient. We further summarize the methods of retrieving sperm, storing, and freezing rare sperm. We reviewed different methods of gamete artificial activation and discussed the feasibility of ROSI for sterile KS patients who absolutely lack sperm. The activation of eggs in the process of intracytoplasmic sperm injection and non-invasive PGD are urgently needed to prevent the birth of KS infants.
Conclusion: The integrated strategies will pave the way for the establishment of ART treatment approaches and improve the clinical outcome for KS patients.
Keywords: Administration strategy; Fertility preservation; Klinefelter syndrome; Single sperm cryopreservation; TESE.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Nielsen J, Wohlert M. Chromosome abnormalities found among 34,910 newborn children: results from a 13-year incidence study in Arhus, Denmark. Hum Genet. 1991;87(1):81–83. - PubMed
-
- Abramsky L, Chapple J. 47,XXY (Klinefelter syndrome) and 47,XYY: estimated rates of and indication for postnatal diagnosis with implications for prenatal counselling. Prenat Diagn. 1997;17(4):363–368. - PubMed
Publication types
MeSH terms
Grants and funding
- 81672562/National Natural Science Foundation of China
- 81872111/National Natural Science Foundation of China
- 81370074/National Natural Science Foundation of China
- 81902630/National Natural Science Foundation of China
- 19XD1423100/Shanghai Municipal Science and Technology Committee of Shanghai outstanding academic leaders plan
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
