

Dabigatran Dual Therapy vs Warfarin Triple Therapy Post-Percutaneous Coronary Intervention in Patients with Atrial Fibrillation With/Without a Proton Pump Inhibitor: A Pre-Specified Analysis of the RE-DUAL PCI Trial
- PMID: 32562206
- PMCID: PMC7320045
- DOI: 10.1007/s40265-020-01323-x
Dabigatran Dual Therapy vs Warfarin Triple Therapy Post-Percutaneous Coronary Intervention in Patients with Atrial Fibrillation With/Without a Proton Pump Inhibitor: A Pre-Specified Analysis of the RE-DUAL PCI Trial
Abstract
Background and objective: In patients with atrial fibrillation following percutaneous coronary intervention, if a proton pump inhibitor is used, could that allow the use of warfarin triple therapy, or is there additional reduction in bleeding while using it with dual therapy?
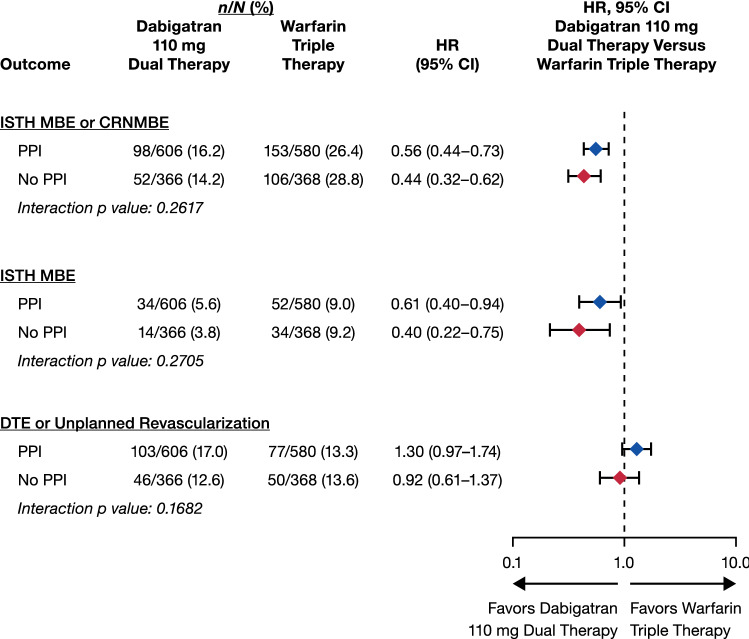
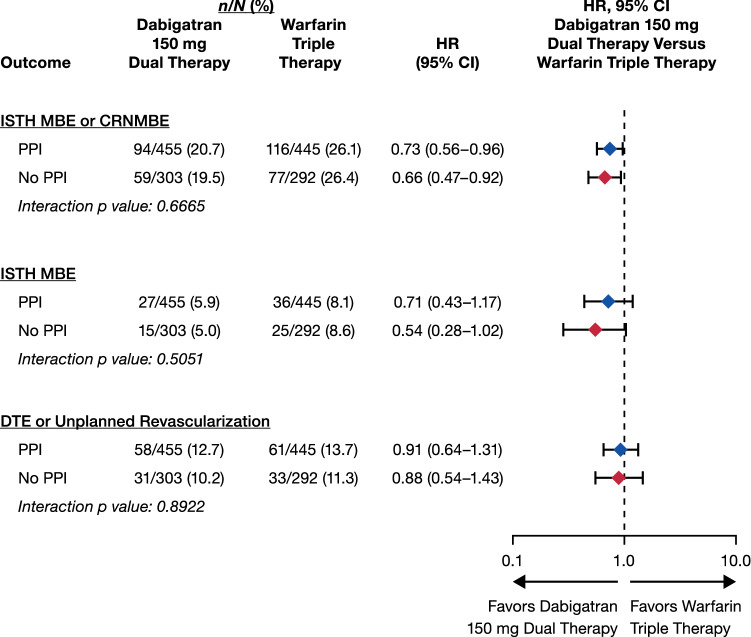
Methods: The RE-DUAL PCI trial randomized 2725 patients with atrial fibrillation post-percutaneous coronary intervention to dabigatran dual therapy (110 or 150 mg twice daily, with clopidogrel or ticagrelor) or warfarin triple therapy (with clopidogrel or ticagrelor, and aspirin for 1-3 months). This prespecified subgroup analysis evaluated risks of a first major bleeding event or clinically relevant non-major bleeding event, all gastrointestinal bleeding, and a composite efficacy endpoint of all-cause mortality/thromboembolic event or unplanned revascularization according to baseline use of a proton pump inhibitor.
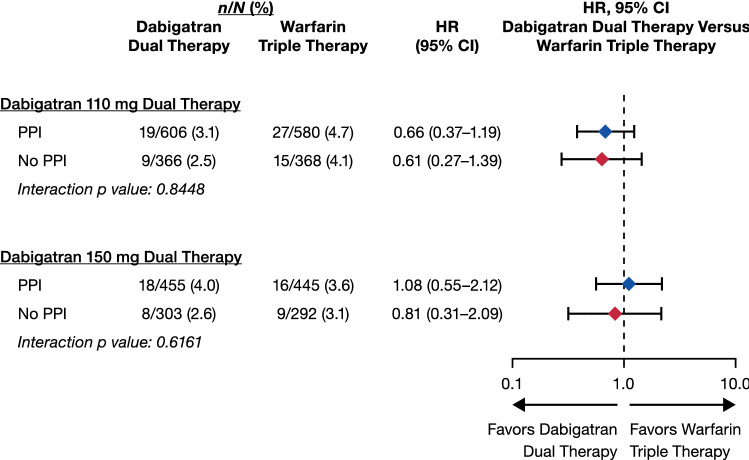
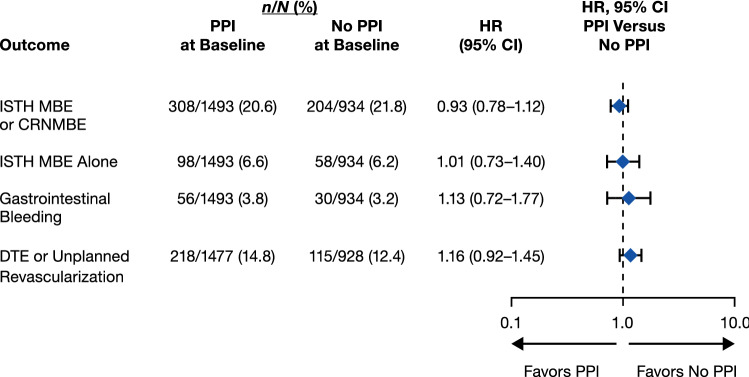
Results: Of 2678 analyzed patients, 1641 (61.3%) were receiving a proton pump inhibitor at baseline. Dabigatran 110 and 150 mg dual therapy reduced the risk of major bleeding events or clinically relevant non-major bleeding events vs warfarin triple therapy regardless of proton pump inhibitor use, with comparable risk of the composite efficacy endpoint (all interaction p values > 0.05). For gastrointestinal bleeding, no interaction was observed between study treatment and proton pump inhibitor use (interaction p values 0.84 and 0.62 for dabigatran 110 and 150 mg dual therapy, respectively, vs warfarin triple therapy).
Conclusions: Dabigatran 110 and 150 mg dual therapy reduced the risk of major bleeding events or clinically relevant non-major bleeding events vs warfarin triple therapy, regardless of proton pump inhibitor use at baseline, in patients with atrial fibrillation who underwent percutaneous coronary intervention. Risk of the composite efficacy endpoint appeared to be similar for dabigatran dual therapy vs warfarin triple therapy in patients receiving/not receiving a proton pump inhibitor. CLINICALTRIALS.
Gov unique identifier: NCT02164864.
Conflict of interest statement
José C. Nicolau has received research grants from CSL Behring, Sanofi, AstraZeneca, Bristol-Myers Squibb, Viforpharma, Dalcorpharma, Janssen, and Novartis; has served as a consultant/advisory board member for Bayer, Merck, Novartis, Sanofi, Servier, Amgen, and AstraZeneca; and a steering committee member for Eisai, Boehringer Ingelheim, AstraZeneca, Sanofi, CSL Behring, Viforpharma, and Dalcorpharma. Deepak L. Bhatt discloses the following relationships: Advisory Board: Cardax, Cereno Scientific, Elsevier Practice Update Cardiology, Medscape Cardiology, PhaseBio, Regado Biosciences; Board of Directors: Boston VA Research Institute, Society of Cardiovascular Patient Care, TobeSoft; Chair: American Heart Association Quality Oversight Committee; Data Monitoring Committees: Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), Population Health Research Institute; Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Vice-Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor-in-Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor-in-Chief,
Figures
References
-
- Lip GYH, Collet JP, Haude M, Byrne R, Chung EH, Fauchier L, et al. 2018 Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: a joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA) Europace. 2019;21(2):192–193. doi: 10.1093/europace/euy174. - DOI - PubMed
-
- Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention, 2011 ACCF/AHA guideline for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease, 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction, 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes, and 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery. Circulation. 2016;134(10):e123–e155. doi: 10.1161/CIR.0000000000000404. - DOI - PubMed
-
- Cardoso RN, Benjo AM, DiNicolantonio JJ, Garcia DC, Macedo FY, El-Hayek G, et al. Incidence of cardiovascular events and gastrointestinal bleeding in patients receiving clopidogrel with and without proton pump inhibitors: an updated meta-analysis. Open Heart. 2015;2(1):e000248. doi: 10.1136/openhrt-2015-000248. - DOI - PMC - PubMed
-
- Hulot JS, Collet JP, Silvain J, Pena A, Bellemain-Appaix A, Barthelemy O, et al. Cardiovascular risk in clopidogrel-treated patients according to cytochrome P450 2C19*2 loss-of-function allele or proton pump inhibitor coadministration: a systematic meta-analysis. J Am Coll Cardiol. 2010;56(2):134–143. doi: 10.1016/j.jacc.2009.12.071. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
