

Integrated screening and treatment services for HIV, hypertension and diabetes in Kenya: assessing the epidemiological impact and cost-effectiveness from a national and regional perspective
- PMID: 32562353
- PMCID: PMC7305418
- DOI: 10.1002/jia2.25499
Integrated screening and treatment services for HIV, hypertension and diabetes in Kenya: assessing the epidemiological impact and cost-effectiveness from a national and regional perspective
Abstract
Introduction: As people with HIV age, prevention and management of other communicable and non-communicable diseases (NCDs) will become increasingly important. Integration of screening and treatment for HIV and NCDs is a promising approach for addressing the dual burden of these diseases. The aim of this study was to assess the epidemiological impact and cost-effectiveness of a community-wide integrated programme for screening and treatment of HIV, hypertension and diabetes in Kenya.
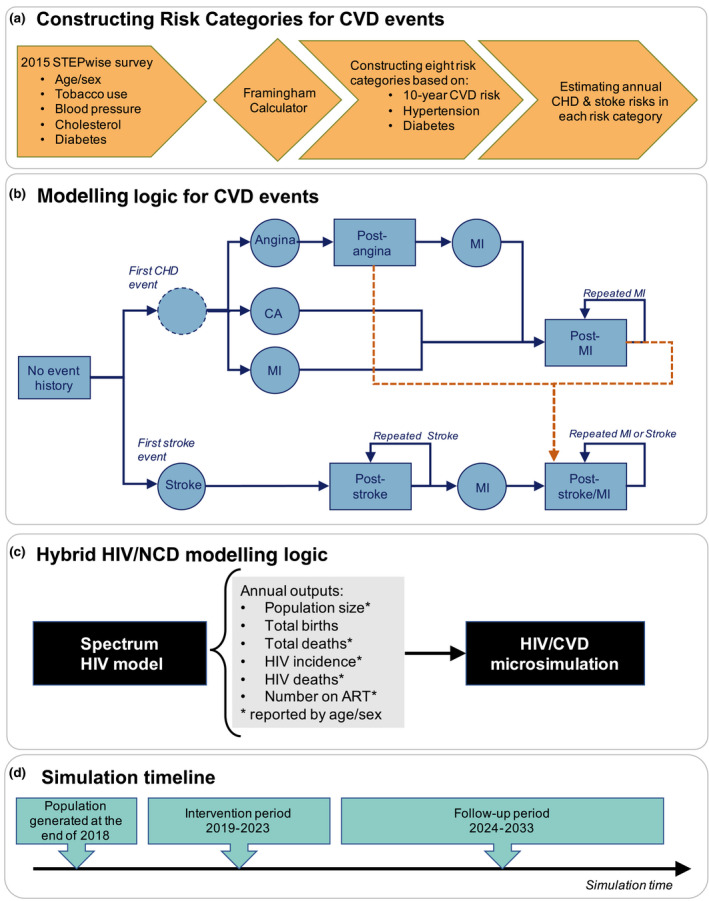
Methods: Coupling a microsimulation of cardiovascular diseases (CVDs) with a population-based model of HIV dynamics (the Spectrum), we created a hybrid HIV/CVD model. Interventions were modelled from year 2019 (baseline) to 2023, and population was followed to 2033. Analyses were carried at a national level and for three selected regions (Nairobi, Coast and Central).
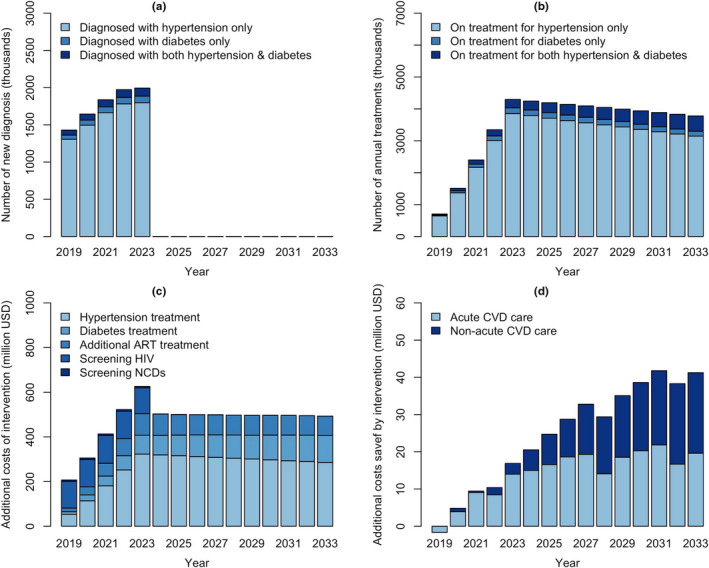
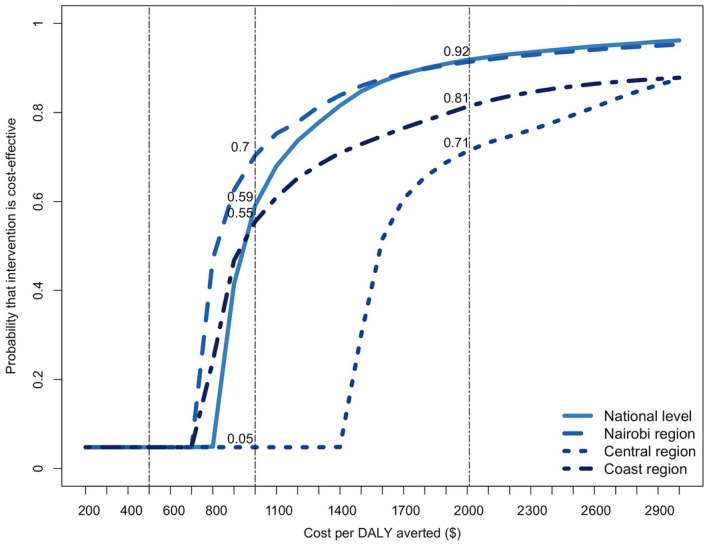
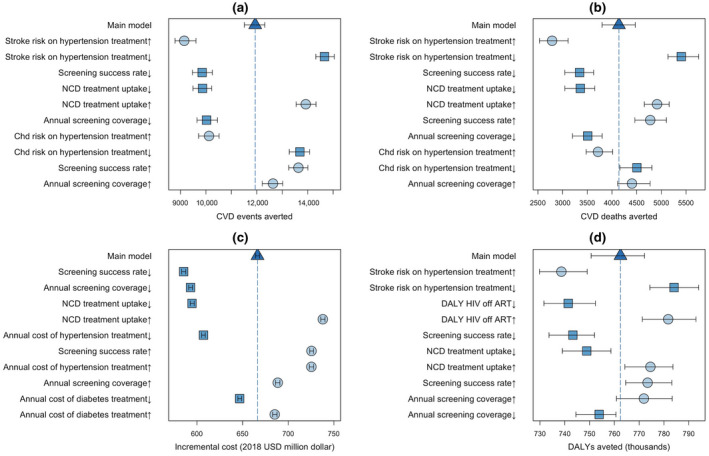
Results: At a national level, the model projected 7.62 million individuals living with untreated hypertension, 692,000 with untreated diabetes and 592,000 individuals in need of ART in year 2018. Improving ART coverage from 68% at baseline to 88% in 2033 reduced HIV incidence by an estimated 64%. Providing NCD treatment to 50% of diagnosed cases from 2019 to 2023 and maintaining them on treatment afterwards could avert 116,000 CVD events and 43,600 CVD deaths in Kenya over the next 15 years. At a regional level, the estimated impact of expanded HIV services was highest in Nairobi region (averting 42,100 HIV infections compared to baseline) while Central region experienced the highest impact of expanded NCD treatment (with a reduction of 22,200 CVD events). The integrated HIV/NCD intervention could avert 7.76 million disability-adjusted-life-years (DALYs) over 15 years at an estimated cost of $6.68 billion ($445.27 million per year), or $860.30 per DALY averted. At a cost-effectiveness threshold of $2,010 per DALY averted, the probability of cost-effectiveness was 0.92, ranging from 0.71 in Central to 0.92 in Nairobi region.
Conclusions: Integrated screening and treatment of HIV and NCDs can be a cost-effective and impactful approach to save lives of people with HIV in Kenya, although important variation exists at the regional level. Containing the substantial costs required for scale-up will be critical for management of HIV and NCDs on a national scale.
Keywords: HIV; Kenya; computer simulation; cost-benefit analysis; diabetes mellitus; hypertension.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- (UNIADS) JUNPoHA . UNIAIDS Data 2019. 2019. [cited 2020 Jan 5]. Available from: https://www.unaids.org/sites/default/files/media_asset/2019‐UNAIDS‐data_...
-
- National AIDS Control Council . Kenya HIV Estimates Report 2018. 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
