

Patient satisfaction after orthognathic surgery: a 3 year follow-up of 60 high-angle Class II individuals
- PMID: 32562420
- PMCID: PMC8023362
- DOI: 10.1093/ejo/cjaa038
Patient satisfaction after orthognathic surgery: a 3 year follow-up of 60 high-angle Class II individuals
Abstract
Background and objectives: High-angle Class II malocclusion is considered challenging to treat to a stable result and, although studies report treatment outcome in terms of morphology, patient satisfaction has not been addressed. The objectives of the present study were to examine patients' motives for treatment and satisfaction with the results.
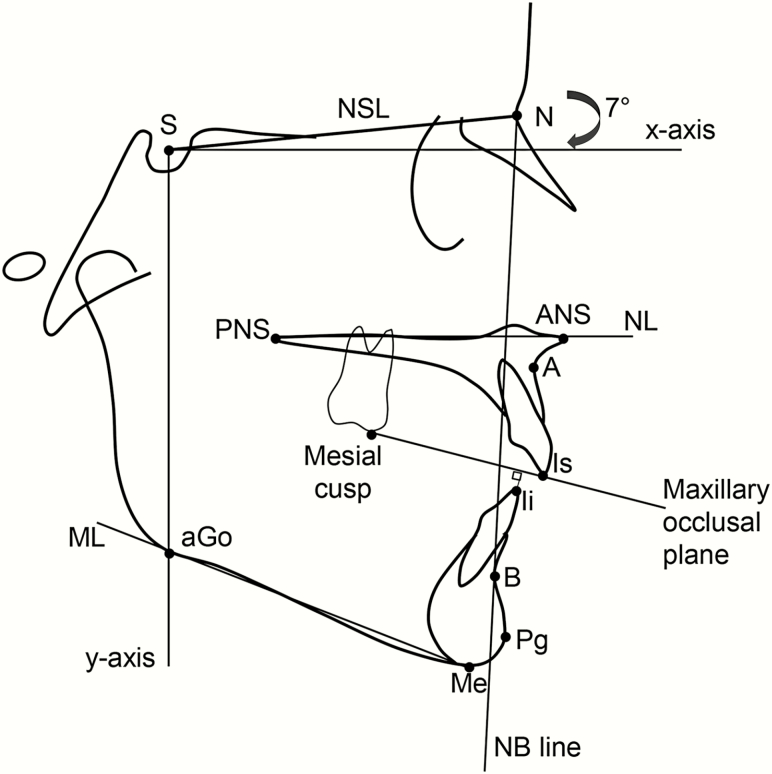
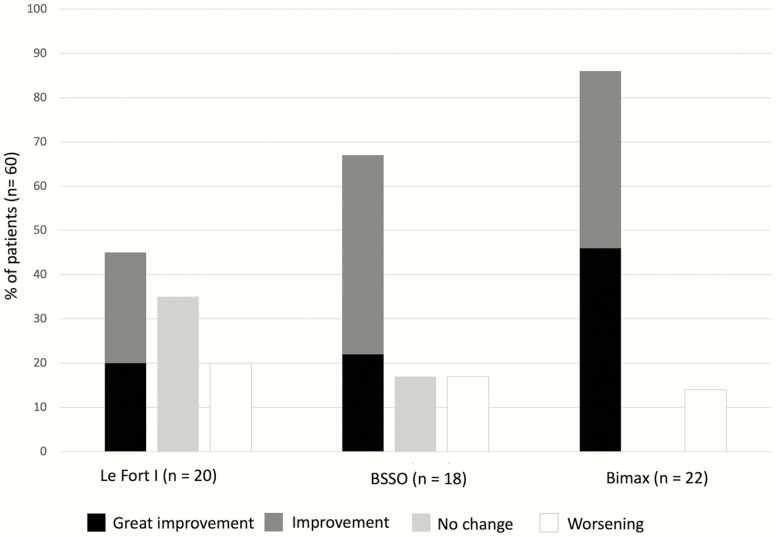
Material and methods: A structured questionnaire was distributed 3 years post-operatively to 93 consecutively treated patients with an initial diagnosis of mandibular-plane angle (ML/NSL) ≥34.0 degrees and ANB angle ≥4.0 degrees. Three surgical subsamples were defined: one-piece Le Fort I, bilateral sagittal split osteotomy, or a combination of the two (Bimax). Lateral cephalometric radiographs were used to assess morphological characteristics and post-treatment changes.
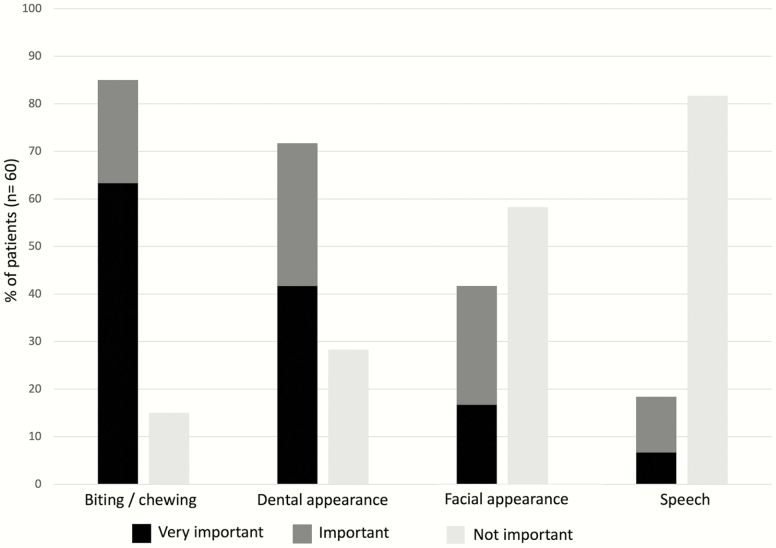
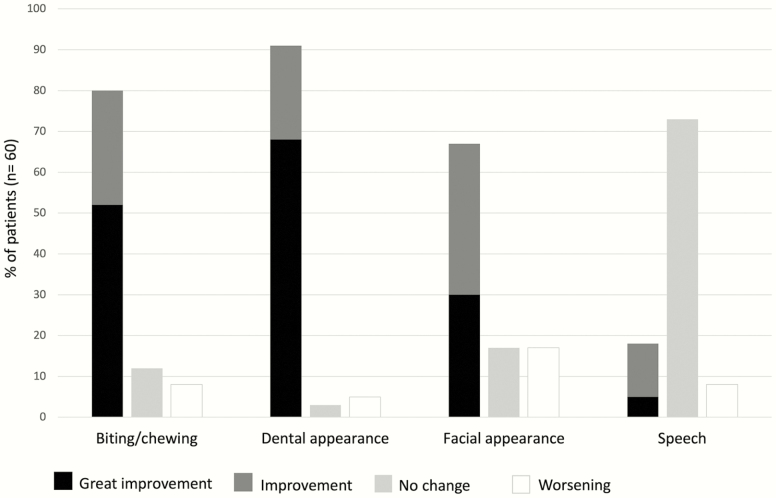
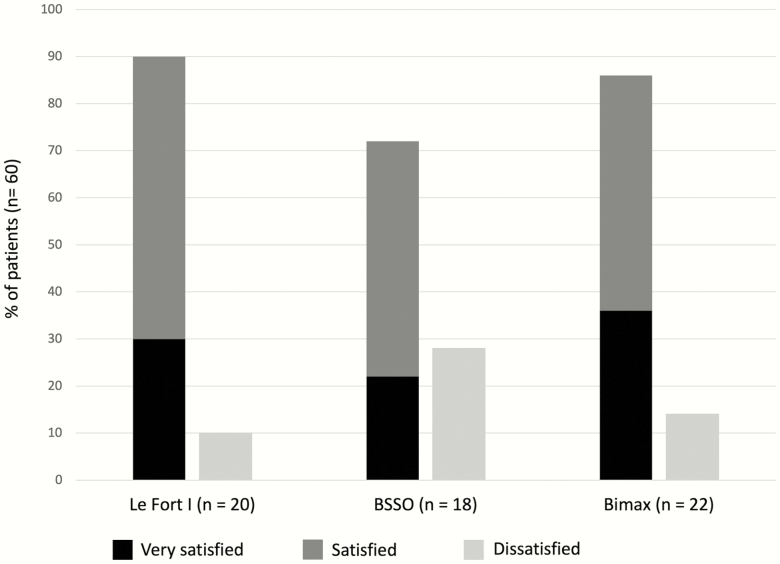
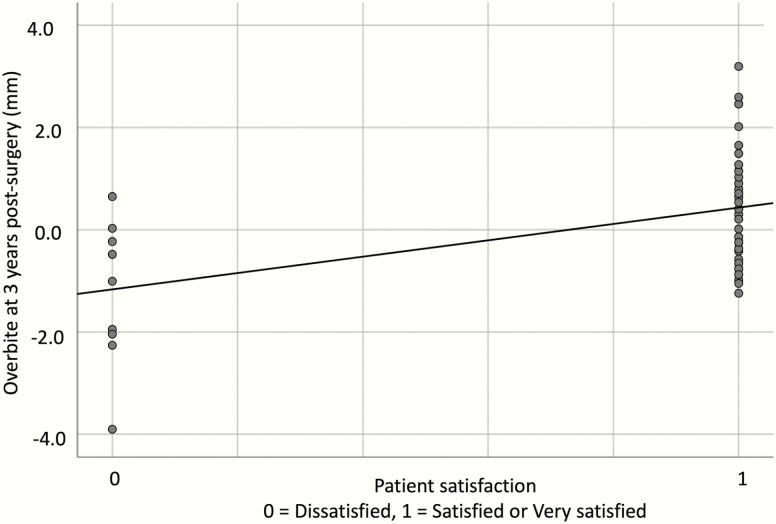
Results: Questionnaire participation was 69.8 per cent. The most frequently reported motives for seeking treatment were to improve oral function (85.0 per cent) and dental appearance (71.7 per cent). Thirty per cent were very satisfied, 53.3 per cent were satisfied, and 16.7 per cent were dissatisfied with the overall treatment result. Dissatisfaction was associated with a persisting post-treatment anterior open bite (AOB), horizontal relapse at B point, and with sensory impairment.
Conclusions and implications: A higher rate of dissatisfaction was found than what has usually been reported for othognathic surgical patients, and this was associated with a persisting AOB. In addition, mandibular relapse and impaired sensory function were related to dissatisfaction and are associated with mandibular surgery. Prospective high-angle Class II patients should be comprehensively informed about the unpredictability of treatment outcomes in terms of occlusion and facial appearance.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Orthodontic Society.
Figures
References
-
- Proffit, W.R., Turvey, T.A. and Phillips, C. (1996) Orthognathic surgery: a hierarchy of stability. The International Journal of Adult Orthodontics and Orthognathic Surgery, 11, 191–204. - PubMed
-
- Mobarak, K.A., Espeland, L., Krogstad, O. and Lyberg, T. (2001) Mandibular advancement surgery in high-angle and low-angle class II patients: different long-term skeletal responses. American Journal of Orthodontics and Dentofacial Orthopedics, 119, 368–381. - PubMed
-
- Borstlap, W.A., Stoelinga, P.J., Hoppenreijs, T.J. and van’t Hof, M.A. (2004) Stabilisation of sagittal split advancement osteotomies with miniplates: a prospective, multicentre study with two-year follow-up. Part II. Radiographic parameters. International Journal of Oral and Maxillofacial Surgery, 33, 535–542. - PubMed
-
- Douma, E., Kuftinec, M.M. and Moshiri, F. (1991) A comparative study of stability after mandibular advancement surgery. American Journal of Orthodontics and Dentofacial Orthopedics, 100, 141–155. - PubMed
