

Clinical-Grade Detection of Microsatellite Instability in Colorectal Tumors by Deep Learning
- PMID: 32562722
- PMCID: PMC7578071
- DOI: 10.1053/j.gastro.2020.06.021
Clinical-Grade Detection of Microsatellite Instability in Colorectal Tumors by Deep Learning
Abstract
Background & aims: Microsatellite instability (MSI) and mismatch-repair deficiency (dMMR) in colorectal tumors are used to select treatment for patients. Deep learning can detect MSI and dMMR in tumor samples on routine histology slides faster and less expensively than molecular assays. However, clinical application of this technology requires high performance and multisite validation, which have not yet been performed.
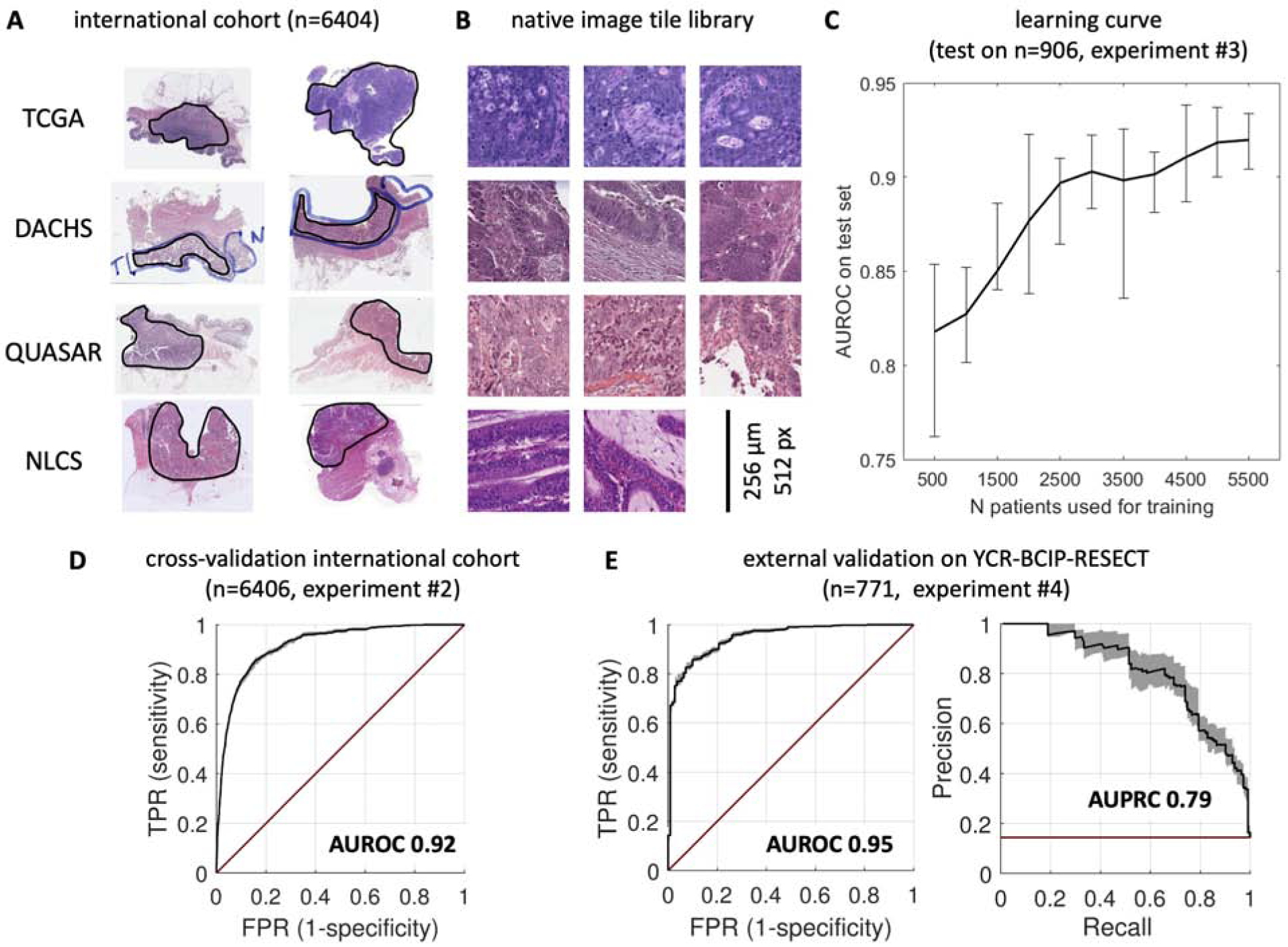
Methods: We collected H&E-stained slides and findings from molecular analyses for MSI and dMMR from 8836 colorectal tumors (of all stages) included in the MSIDETECT consortium study, from Germany, the Netherlands, the United Kingdom, and the United States. Specimens with dMMR were identified by immunohistochemistry analyses of tissue microarrays for loss of MLH1, MSH2, MSH6, and/or PMS2. Specimens with MSI were identified by genetic analyses. We trained a deep-learning detector to identify samples with MSI from these slides; performance was assessed by cross-validation (N = 6406 specimens) and validated in an external cohort (n = 771 specimens). Prespecified endpoints were area under the receiver operating characteristic (AUROC) curve and area under the precision-recall curve (AUPRC).
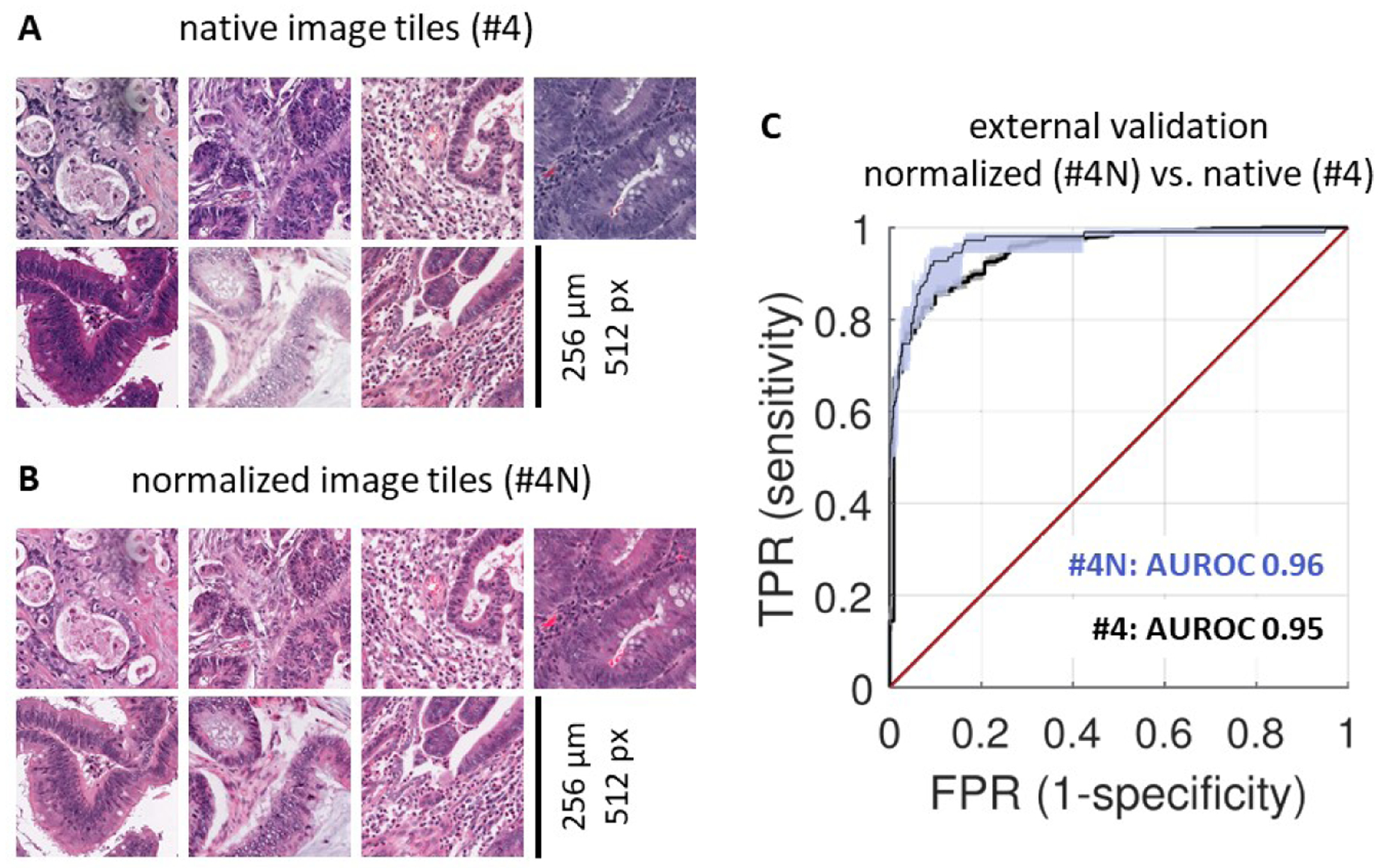
Results: The deep-learning detector identified specimens with dMMR or MSI with a mean AUROC curve of 0.92 (lower bound, 0.91; upper bound, 0.93) and an AUPRC of 0.63 (range, 0.59-0.65), or 67% specificity and 95% sensitivity, in the cross-validation development cohort. In the validation cohort, the classifier identified samples with dMMR with an AUROC of 0.95 (range, 0.92-0.96) without image preprocessing and an AUROC of 0.96 (range, 0.93-0.98) after color normalization.
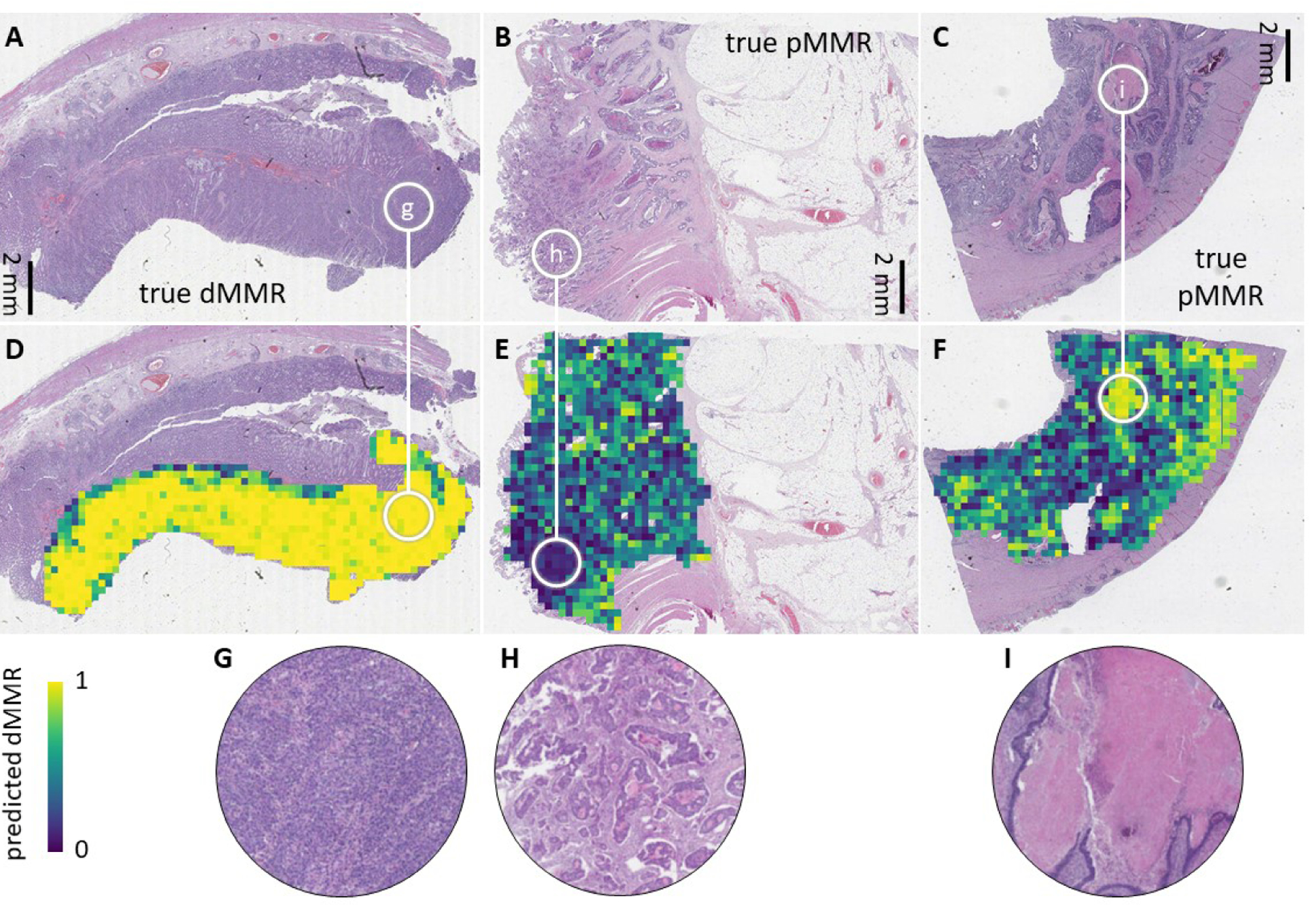
Conclusions: We developed a deep-learning system that detects colorectal cancer specimens with dMMR or MSI using H&E-stained slides; it detected tissues with dMMR with an AUROC of 0.96 in a large, international validation cohort. This system might be used for high-throughput, low-cost evaluation of colorectal tissue specimens.
Keywords: Lynch syndrome; biomarker; cancer immunotherapy; mutation.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Colorectal Cancer: Microsatellite Instability/Mismatch Repair Testing in the Era of Digital Pathology.Gastroenterology. 2020 Oct;159(4):1235-1237. doi: 10.1053/j.gastro.2020.08.008. Epub 2020 Aug 13. Gastroenterology. 2020. PMID: 32800777 No abstract available.
References
-
- Luchini C, Bibeau F, Ligtenberg MJL, et al. ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: a systematic review-based approach. Ann Oncol 2019;30:1232–1243. - PubMed
-
- Kather JN, Halama N, Jaeger D. Genomics and emerging biomarkers for immunotherapy of colorectal cancer. Semin Cancer Biol 2018;52:189–197. - PubMed
-
- Anon. Molecular testing strategies for Lynch syndrome in people with colorectal cancer - NICE Guidance. Available at: https://www.nice.org.uk/guidance/dg27/chapter/1-Recommendations [Accessed November 13, 2019].
-
- Stjepanovic N, Moreira L, Carneiro F, et al. Hereditary gastrointestinal cancers: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol 2019;30:1558–1571. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
